
The California WIC form is a two-page referral document completed by licensed healthcare providers. It connects pregnant, postpartum, and breastfeeding women to the Women, Infants, and Children (WIC) Program for nutritional counseling and supplemental food benefits in California.
What You Need to Fill Out the California WIC Form
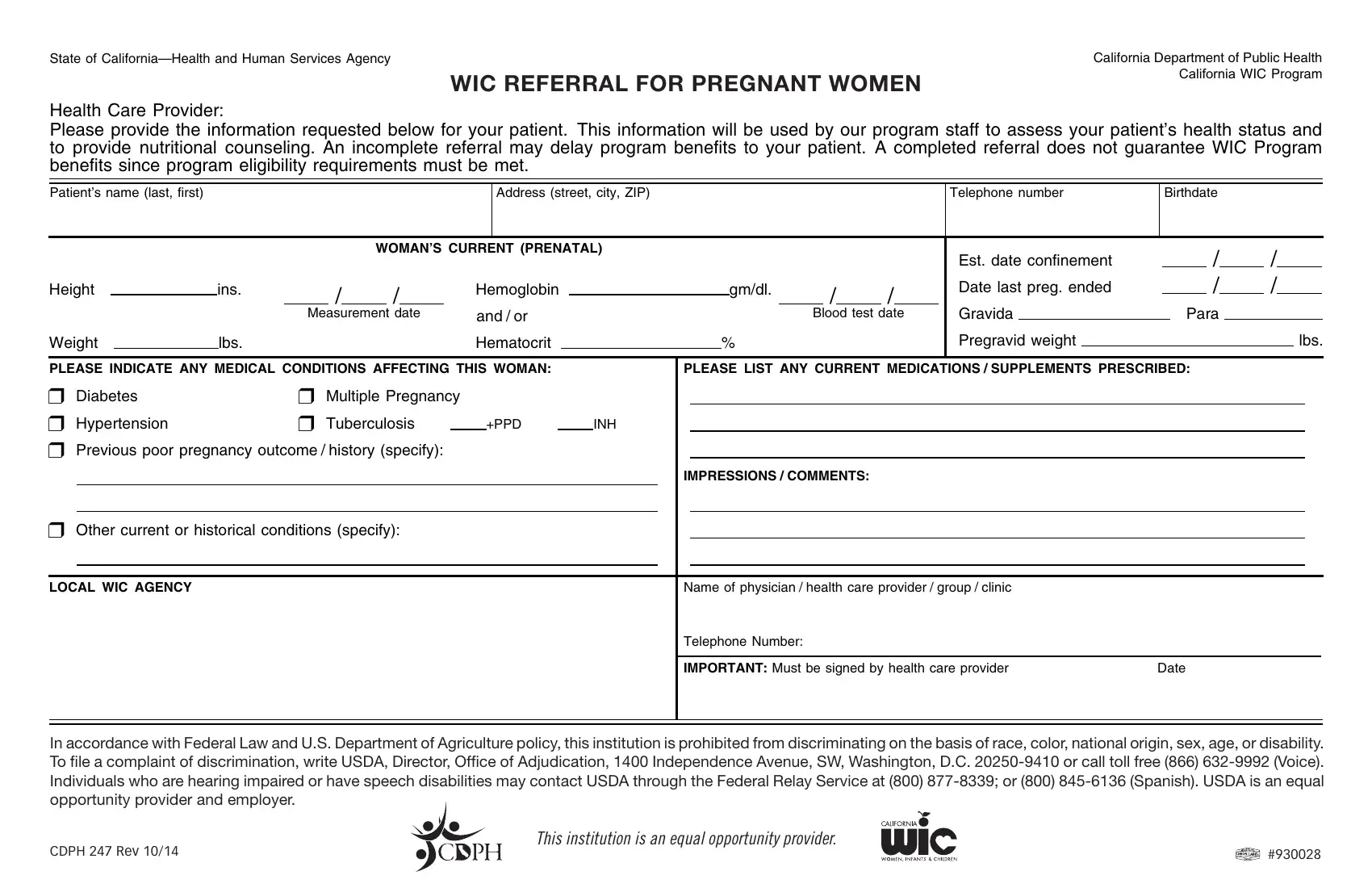
Gather these items before completing the form:
- Patient's full legal name and date of birth
- Patient's home address and phone number
- Current medical diagnoses and health conditions
- List of prescribed medications and nutritional supplements
- Healthcare provider's name, license number, and facility address
How to Complete the California WIC Referral Form
Follow these steps to fill out the form correctly:
- Patient Information: Enter the patient's full name, date of birth, address, and phone number. For pregnant patients, include the estimated due date.
- Health Status: Document the patient's current medical conditions. Include diagnoses related to nutritional health, such as anemia, gestational diabetes, or low birth weight risk.
- Nutritional Needs: Describe any nutritional deficiencies, dietary restrictions, or special requirements that indicate the patient needs WIC support.
- Medications and Supplements: List all current prescription medications and supplements, including dosage and frequency.
- Provider Certification: Sign and date the form. Include your professional license number and the name of your medical practice or facility.
- Submission: Give the completed California WIC form to the patient to bring to their nearest WIC clinic, or submit it directly to the local WIC program office.
Frequently Asked Questions About the California WIC Form
Does completing the form guarantee WIC benefits?
No. The referral form starts the application process. Patients must meet California's WIC eligibility requirements, including income limits and assessed nutritional risk, to receive program benefits.
Who is eligible for the California WIC Program?
The California WIC Program serves pregnant women, postpartum women (up to 6 months after delivery), breastfeeding women (up to 12 months), and infants and children up to age 5 who have a documented nutritional risk and meet income guidelines.
What benefits does the WIC program provide?
WIC benefits include supplemental nutritious foods, nutrition education and counseling, breastfeeding support, and referrals to healthcare and social services tailored to each participant.
Related Prenatal and Health Forms
Healthcare providers working with prenatal patients may also need the prenatal record form to document complete pregnancy health history, or the ACOG prenatal form for standardized obstetric documentation. Registered dietitians can use the nutritionist assessment form to record dietary evaluations alongside the WIC referral.