Encouraging a healthy lifestyle among its customers, Dartmouth College and Cigna have teamed up to offer a generous fitness reimbursement program, a significant boon for those under the CIGNA Medical Plan. This initiative allows individuals and their families to be reimbursed for up to $200 per calendar year for fees associated with qualified fitness facility memberships or exercise classes. Whether you prefer working out at a full-service gym, taking classes at a yoga studio, or engaging in activities at a martial arts center, among others, this program supports a wide array of physical fitness facilities. To qualify, participants must engage in fitness activities twice a week for a minimum of 10 out of 20 weeks. Compliance with the program's requirements involves submitting a Fitness Reimbursement Form complete with a fitness reimbursement log card endorsed by an instructor or facility, alongside dated receipts or bank statements evidencing payment. Timeliness is also crucial, as submissions must be made within 90 days following the calendar year's end to take advantage of this benefit. As participants gear up to maintain or kick start their fitness journeys, this program not only incentivizes physical well-being but also eases the financial burden associated with keeping fit.
| Question | Answer |
|---|---|
| Form Name | Cigna Gym Reimbursement Form |
| Form Length | 3 pages |
| Fillable? | Yes |
| Fillable fields | 142 |
| Avg. time to fill out | 29 min 13 sec |
| Other names | cigna fitness program, cigna gym reimbursement 2021, does cigna cover gym memberships, cigna gym reimbursement form |
Dartmouth College/Cigna Fitness Benefit
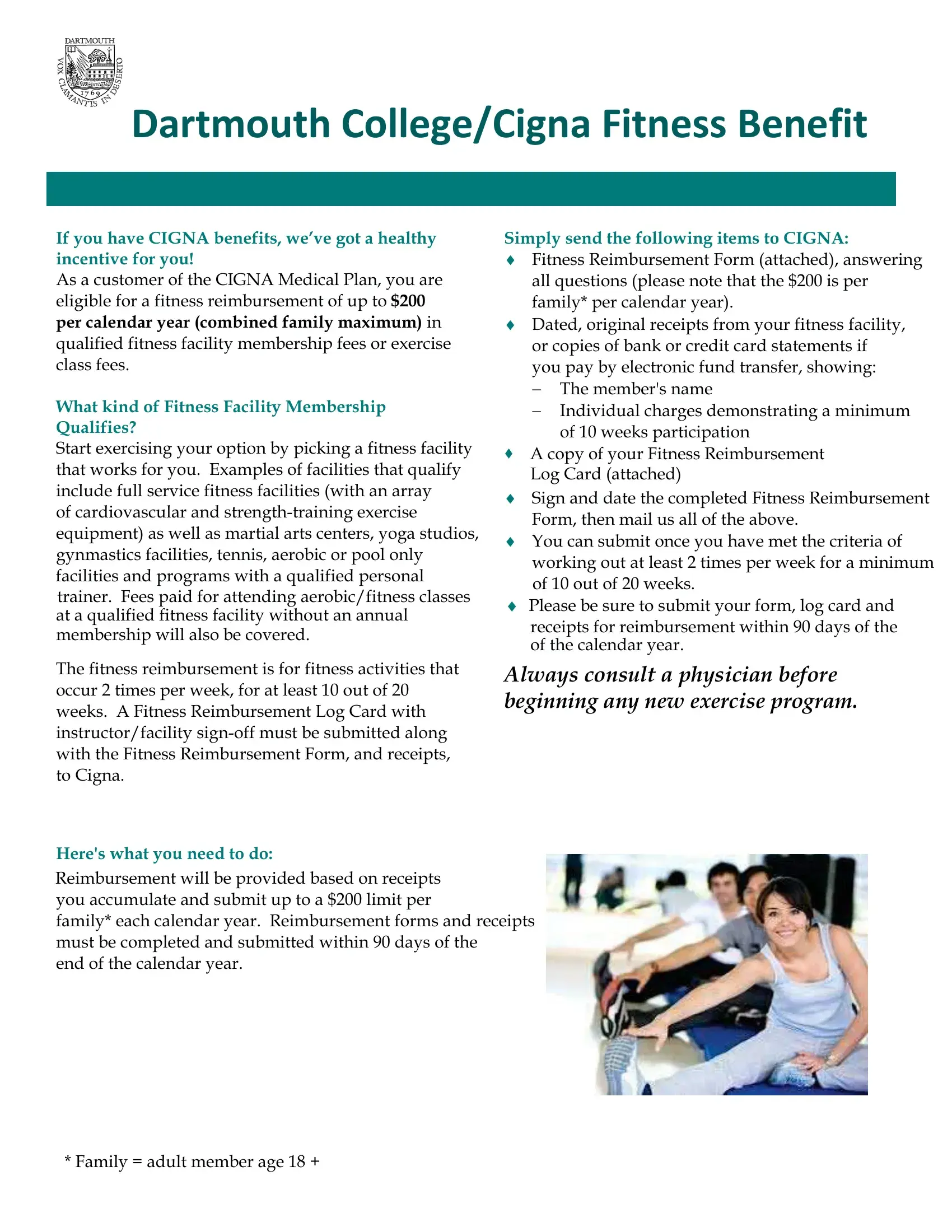
If you have CIGNA benefits, we’ve got a healthy incentive for you!
As a customer of the CIGNA Medical Plan, you are eligible for a fitness reimbursement of up to $200 per calendar year (combined family maximum) in qualified fitness facility membership fees or exercise class fees.
What kind of Fitness Facility Membership Qualifies?
Start exercising your option by picking a fitness facility that works for you. Examples of facilities that qualify include full service fitness facilities (with an array
of cardiovascular and
The fitness reimbursement is for fitness activities that occur 2 times per week, for at least 10 out of 20 weeks. A Fitness Reimbursement Log Card with instructor/facility
Here's what you need to do:
Simply send the following items to CIGNA:
iFitness Reimbursement Form (attached), answering all questions (please note that the $200 is per family* per calendar year).
iDated, original receipts from your fitness facility, or copies of bank or credit card statements if you pay by electronic fund transfer, showing:
The member's name
Individual charges demonstrating a minimum of 10 weeks participation
A copy of your Fitness Reimbursement
Log Card (attached)
iSign and date the completed Fitness Reimbursement Form, then mail us all of the above.
iYou can submit once you have met the criteria of working out at least 2 times per week for a minimum of 10 out of 20 weeks.
Please be sure to submit your form, log card and
receipts for reimbursement within 90 days of the of the calendar year.
Always consult a physician before beginning any new exercise program.
Reimbursement will be provided based on receipts you accumulate and submit up to a $200 limit per
family* each calendar year. Reimbursement forms and receipts must be completed and submitted within 90 days of the
end of the calendar year.
* Family = adult member age 18 +
Dartmouth College/Cigna Fitness Reimbursement Form
PLEASE PRINT ALL INFORMATION CLEARLY
CIGNA ID Number |
Last Name |
First Name |
Middle Initial |
|
|
|
|
Address ‐ Number & Street |
City |
State |
Zip Code |
|
|
|
|
Employer's Name Dartmouth College |
|
|
|
Gender: |
Male |
Female |
Date of Birth (MM/DD/YYYY):
WHEN TO SUBMIT FORM
After you have met the criteria of working out at least 2 times per week for a minimum of 10 out of 20 weeks After you have collected $200 in receipts from qualified fitness facilities
Once per calendar year
Please be sure to submit your reimbursement form, log card and receipts for reimbursement within 90 days of the end of
the calendar year.
CLUB/CLASS INFORMATION REQUIRED (Attach itemized receipts)
Name and Address of fitness facility
Dates of Service
Amount Charged
TOTAL NUMBER OF RECEIPTS ATTACHED: |
|
TOTAL CHARGES: $ |
|
|
|
|
|
All Fitness Benefit payments will be sent to the Customer's address on file.
CERTIFICATION AND AUTHORIZATION (This form must be signed and dated below)
I authorize the release of any information to CIGNA about my health club membership. I certify that the information provided in support of this submission is complete and correct and that I have not previously submitted for these services.
Cigna Customer Signature/Member's Signature: |
|
Date: |
Please mail to the below address. Please also allow up to four weeks for processing.
CIGNA
Attn: Debra Sargent
2 College Park Drive
Hooksett, NH 03106
Note: If services are denied, a denial letter will be sent to the customer’s home address. Please be sure to keep copies of your form and receipts, we will not return any receipts or claims forms.
Dartmouth College / Cigna Fitness Reimbursement Log Card
Name:________________________________________________________________________________
Address:______________________________________________________________________________
Phone Number:_________________________________________________________________________
Cigna ID #:____________________________________________________________________________
All workouts must be logged in the same calendar year.
To qualify, you must exercise a minimum of two times per week for 10 out of 20 weeks.
(To meet exercise requirements within a calendar year, this log card must be
started no later than October 22nd of a given calendar year).
Return Log Card along with Fitness Reimbursement Form and Receipts to:
Cigna Healthcare – Attention: Debra Sargent
2 College Park Drive
Hooksett, NH 03106
|
FITNESS LOG |
|
|
Record daily exercise here. |
|
|
|
|
|||||||
|
CARD |
|
|
|
(Fitness Facility Employee / Instructor confirmation initials go inside the box.) |
|
|||||||||
|
Record dates at the |
|
Day 1 |
|
|
|
|
Day 2 |
|||||||
|
beginning of each |
|
|
|
|
|
|
|
|
|
|
||||
|
week here |
|
|
Exercise |
|
Initial |
|
Exercise |
|
|
Initial |
|
|||
|
Week 1 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 2 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 3 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 4 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 5 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 6 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 7 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 8 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 9 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 10 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 11 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 12 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 13 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 14 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 15 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 16 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 17 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 18 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 19 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Week 20 |
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Electronic copies verifying attendance, printed on fitness facility letterhead, will also be accepted.