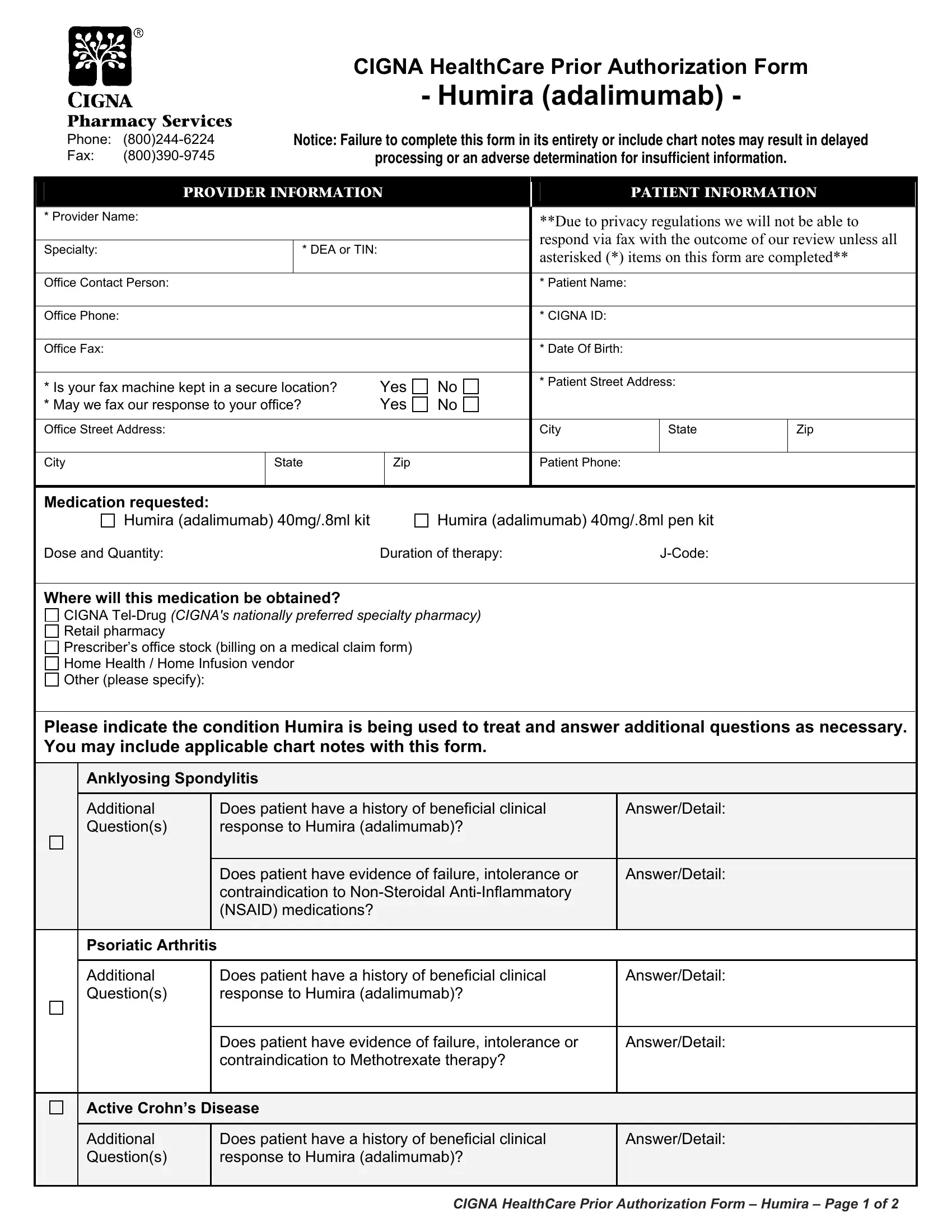
In today's healthcare landscape, navigating the specifics of medication coverage can be a daunting task for both healthcare providers and patients. Among the various forms and procedures, the Cigna Health Assessment form for Humira (adalimumab) stands out due to its comprehensive approach towards prior authorization. This form serves a critical bridge in ensuring patients receive the necessary medication by meticulously detailing requirements ranging from provider and patient information, medication specifics, to detailed medical history and current treatment regimens. Designed to streamline the decision-making process for drug coverage, it prompts the provider to document the patient's medical condition, prior treatments, and the rationale behind choosing Humira. Additionally, stipulations around secure faxing procedures reflect a keen sensitivity to privacy concerns, ensuring compliance with regulations and safeguarding patient information. The form also facilitates consideration of a patient's response to Humira, making it a vital tool for continued therapy assessments. As part of Cigna's pharmacy services, this prior authorization form embodies the intricate balance between regulatory requirements, clinical judgement, and patient care—ultimately influencing the timely access to essential medications for conditions like Anklyosing Spondylitis, Psoriatic Arthritis, Crohn’s Disease, and more.
| Question | Answer |
|---|---|
| Form Name | Cigna Health Assessment Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cigna humira pa form, cigna health risk assessment form, cigna prior authorization form, cigna humira form |
Pharmacy Services
Phone:
Fax:
CIGNA HealthCare Prior Authorization Form
- Humira (adalimumab) -
Notice: Failure to complete this form in its entirety or include chart notes may result in delayed
processing or an adverse determination for insufficient information.
|
|
PROVIDER INFORMATION |
|
|
PATIENT INFORMATION |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* Provider Name: |
|
|
|
|
|
|
**Due to privacy regulations we will not be able to |
|
|||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
respond via fax with the outcome of our review unless all |
|
|||
|
Specialty: |
|
|
* DEA or TIN: |
|
|
|
|
||||
|
|
|
|
|
|
asterisked (*) items on this form are completed** |
|
|||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Contact Person: |
|
|
|
|
|
|
* Patient Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Phone: |
|
|
|
|
|
|
* CIGNA ID: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Fax: |
|
|
|
|
|
|
* Date Of Birth: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* Is your fax machine kept in a secure location? |
Yes |
No |
* Patient Street Address: |
|
|
||||||
|
|
|
|
|
|
|||||||
|
* May we fax our response to your office? |
Yes |
No |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Street Address: |
|
|
|
|
|
|
City |
|
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip |
|
Patient Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Medication requested: |
|
|
|
|
|
|
|
|
|||
|
Humira (adalimumab) 40mg/.8ml kit |
|
|
Humira (adalimumab) 40mg/.8ml pen kit |
|
|
||||||
|
Dose and Quantity: |
|
|
|
Duration of therapy: |
|
|
|
|
|||
Where will this medication be obtained?
CIGNA
Retail pharmacy
Prescriber’s office stock (billing on a medical claim form)
Home Health / Home Infusion vendor
Other (please specify):
Please indicate the condition Humira is being used to treat and answer additional questions as necessary. You may include applicable chart notes with this form.
Anklyosing Spondylitis
Additional Question(s)
|
Does patient have a history of beneficial clinical |
|
|
Answer/Detail: |
|
|
|
|
|
|
|
||
|
response to Humira (adalimumab)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Does patient have evidence of failure, intolerance or |
|
|
Answer/Detail: |
|
|
|
contraindication to |
|
|
|
|
|
|
(NSAID) medications? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Psoriatic Arthritis
Additional Question(s)
Does patient have a history of beneficial clinical |
Answer/Detail: |
|
response to Humira (adalimumab)? |
|
|
|
|
|
Does patient have evidence of failure, intolerance or |
Answer/Detail: |
|
contraindication to Methotrexate therapy? |
|
|
|
|
Active Crohn’s Disease
Additional Question(s)
Does patient have a history of beneficial clinical response to Humira (adalimumab)?
Answer/Detail:
CIGNA HealthCare Prior Authorization Form – Humira – Page 1 of 2
Does patient have evidence of failure, intolerance or contraindication, or inadequate response to conventional therapies (such as aminosalicylate, corticosteroids or immumodulators)?
Answer/Detail:
Rheumatoid Arthritis or Juvenile Idiopathic Arthritis
What is the patient’s diagnosis? |
Rheumatoid Arthritis |
Juvenile Idiopathic Arthritis |
|
|
|
|
|
What is the patient’s current weight? |
|
|
|
|
|||
Does the patient have a history of beneficial clinical response to Humira therapy? |
|||
Yes |
No |
|
|
Please indicate if the patient has had evidence of failure, inadequate response, intolerance or contraindication to any of the following
Methotrexate |
Azathioprine |
Gold |
Hydroxychloroquine |
Penacillamine |
Sulfasalazine |
Other (please specify): |
|
Which of the following methods was used to measure the patient’s disease progression PRIOR to therapy on Humira? (Check all that apply):
Health Assessment Questionnaire Disease Index |
Visual Analogue scale (VAS) |
Likert scales of global response to pain by the patient/doctor |
Global Arthritis Score (GAS) |
Clinical Disease Activity Index (CDAI) |
Simplified Disease Activity Index (SDAI) |
Progression of radiographic damage of involved joints |
Disease Activity Scale (DAS) score |
Disease Activity Score based on
If this is a request for CONTINUED THERAPY (after at least 16 weeks of treatment), has the patient shown beneficial response to treatment with Humira on any of the following measurements? (Check all that showed a beneficial response to Humira therapy):
Health Assessment Questionnaire Disease Index |
Visual Analogue scale (VAS) |
Likert scales of global response to pain by the patient/doctor |
Global Arthritis Score (GAS) |
Clinical Disease Activity Index (CDAI) |
Simplified Disease Activity Index (SDAI) |
Disease Activity Scale (DAS) score
Disease Activity Score based on
Additional pertinent information:
Chronic Plaque Psoriasis
Does patient have a history of beneficial clinical response to Humira (adalimumab)?
Yes
No
Is the patient a candidate for, or have they previously received, systemic therapy (Methotrexate, cyclosporin,
soriatane)? |
Yes |
No |
Is the patient a candidate for, or have they previously received, phototherapy (Narrow and Broad Band UVB, PUVA)?
Yes |
No |
Other (Please specify diagnosis and any additional applicable information)
CIGNA HealthCare’s coverage position on this and other medications may be viewed online at:
http://www.cigna.com/customer_care/healthcare_professional/coverage_positions
Please fax completed form to
Our standard response time for prescription drug coverage requests is
“CIGNA Pharmacy Management” or “CIGNA HealthCare” refer to various operating subsidiaries of CIGNA Corporation. Products and services are provided by these subsidiaries and not by CIGNA Corporation. These subsidiaries include Connecticut General Life Insurance Company, Tel- Drug, Inc.,
V 041510
CIGNA HealthCare Prior Authorization Form – Humira – Page 2 of 2