
What Is the Cigna IVIG Authorization Form?
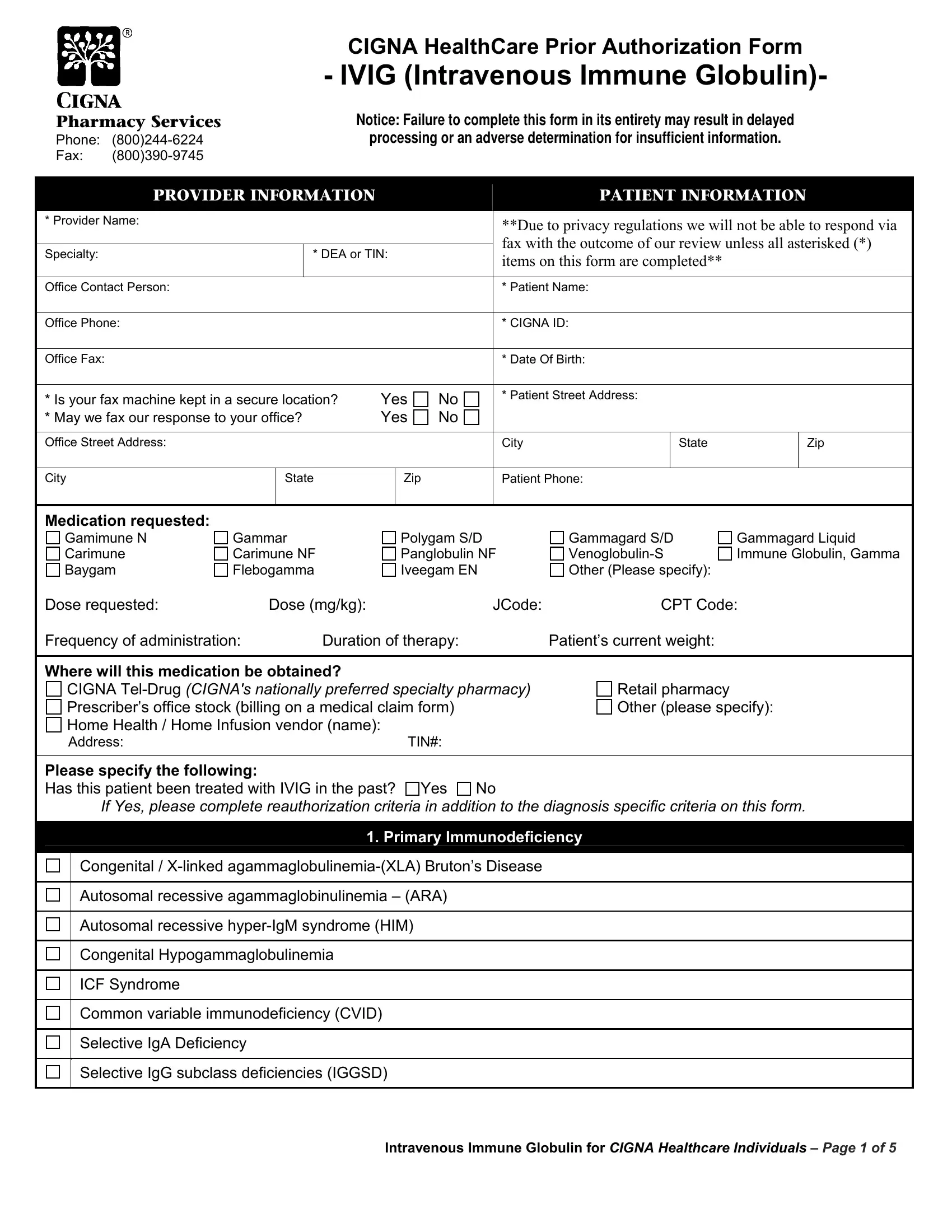
This prior authorization document is submitted to Cigna HealthCare before beginning intravenous immune globulin (IVIG) therapy. Cigna requires this review to confirm that IVIG is medically necessary for the patient's specific diagnosis and that the requested product and dose are appropriate under the plan's coverage criteria. Without an approved authorization, claims for IVIG infusion will typically be denied, even if the treatment is clinically warranted.
Who Needs to Complete This Authorization Request?
Any physician, specialist, or infusion center operating under a patient's Cigna health plan must complete the prior authorization request before the first infusion. This requirement applies whether the treatment will be administered in an outpatient infusion center, a physician's office, or the patient's home. Neurologists, immunologists, hematologists, and rheumatologists are among the specialists who most commonly submit IVIG authorization requests under Cigna plans.
How to Complete the IVIG Prior Authorization Step by Step
Follow these steps to fill out and submit the IVIG authorization request correctly and avoid processing delays:
- Enter full provider information. Include the treating physician's full name, NPI number, medical group affiliation, practice address, direct phone number, and fax number in Section 1. Incomplete or illegible provider details are one of the most frequent reasons authorization requests are returned without review.
- Supply accurate patient demographics. Provide the member's full legal name, Cigna member ID number, date of birth, and insurance group number exactly as they appear on the patient's insurance card. Name mismatches between the form and the insurer's records can delay processing by several business days.
- Identify the IVIG product and dosing plan. Specify the exact brand name (for example, Gamunex-C, Privigen, Octagam, or Panzyga), the requested dose in grams per kilogram of body weight, and the planned infusion frequency. If subcutaneous immune globulin (SCIG) is being substituted, note this in the product field.
- Document the diagnosis and ICD-10 codes. List the primary immunodeficiency or qualifying condition with the corresponding ICD-10 code. Common examples include CVID (D83.9), X-linked agammaglobulinemia (D80.0), acquired hypogammaglobulinemia (D80.1), and CLL-related immunodeficiency (C91.10). For neurological indications such as Guillain-Barre syndrome (G61.0) or chronic inflammatory demyelinating polyneuropathy (G61.81), attach the relevant diagnostic workup results.
- Attach supporting clinical laboratory data. Include the patient's most recent IgG serum level (typically required within the past 12 months for initial requests), vaccine response results to at least two antigens, and records of any prior IVIG treatments including doses and outcomes. Cigna's review team will compare submitted IgG levels against published diagnostic thresholds.
- Complete reauthorization fields for ongoing therapy. For patients already receiving IVIG, document the clinical response to prior treatment cycles, current IgG trough levels, and the rationale for continuing at the same dose. If dose adjustments are requested, provide the clinical justification in the appropriate field.
- Include emergency or expedited review notation if applicable. If the patient's condition requires treatment within 24 to 72 hours, check the expedited review box and attach a brief clinical summary explaining the urgency. Standard review takes 5 to 7 business days; expedited review is typically completed within 24 to 72 hours.
- Obtain physician signature and submit. The treating or ordering physician must sign and date the completed form. Submit via the fax number printed on the form or through the provider portal on Cigna's website. Keep a copy for the patient's medical record.
Common Errors That Delay Authorization Approval
Review this checklist before submitting to avoid the most frequent processing delays:
- Missing or illegible NPI number or provider fax number in Section 1
- Omitting IgG serum level lab results required under primary immunodeficiency criteria
- Failing to specify the requested IVIG brand when multiple products are formulary-listed
- Leaving reauthorization fields blank for patients already receiving ongoing IVIG therapy
- Using an outdated version of the form that does not match current Cigna clinical criteria
- Submitting without the physician's original signature on the final page
Related Cigna and Prior Authorization Forms
Providers managing other Cigna coverage requests or appeals may find these related documents useful:
- Cigna Appeal Form for challenging a prior authorization denial or filing a coverage appeal
- Cigna Form SP1813 for additional Cigna plan coverage and benefits requests
- Aetna Pharmacy Prior Authorization Form for pharmacy benefit authorization requests under Aetna plans