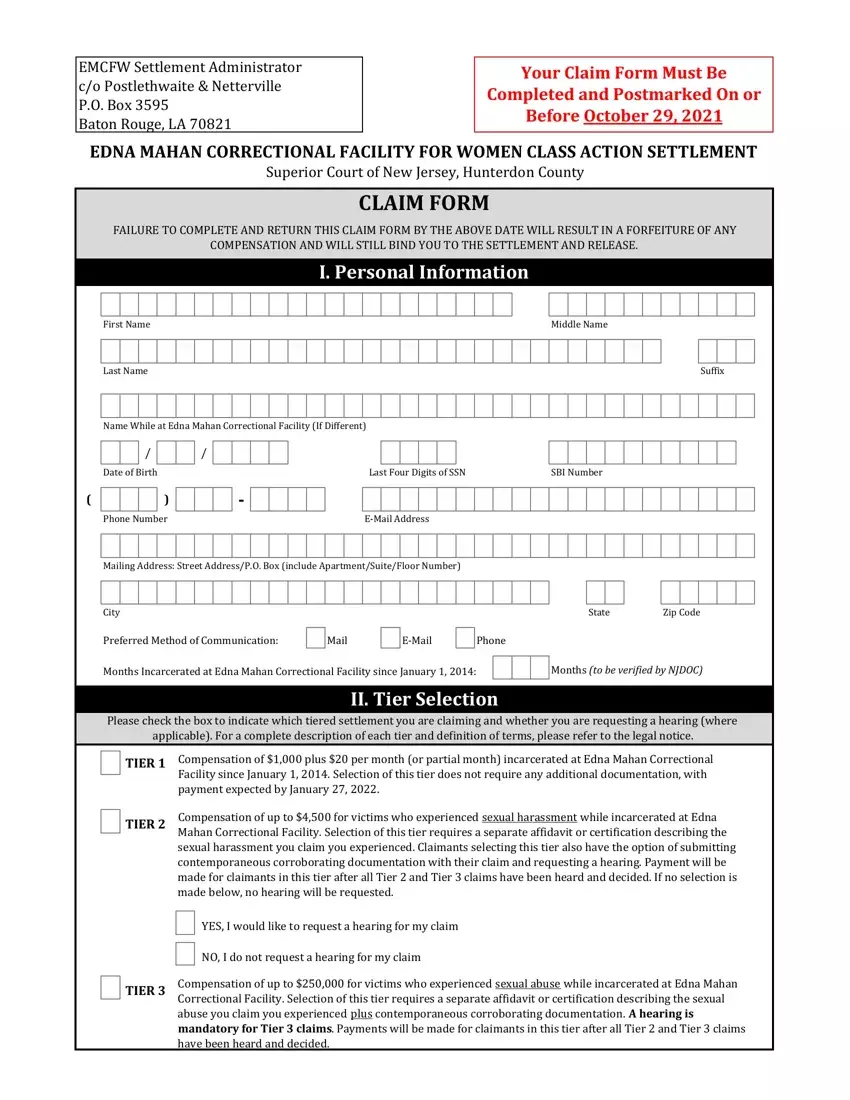
EMCFW Settlement Administrator c/o Postlethwaite & Netterville P.O. Box 3595
Baton Rouge, LA 70821
Your Claim Form Must Be
Completed and Postmarked On or
Before October 29, 2021
EDNA MAHAN CORRECTIONAL FACILITY FOR WOMEN CLASS ACTION SETTLEMENT
Superior Court of New Jersey, Hunterdon County
CLAIM FORM
FAILURE TO COMPLETE AND RETURN THIS CLAIM FORM BY THE ABOVE DATE WILL RESULT IN A FORFEITURE OF ANY
COMPENSATION AND WILL STILL BIND YOU TO THE SETTLEMENT AND RELEASE.
I. Personal Information
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Middle Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Last |
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suffix |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name While |
|
at Edna |
|
Mahan |
|
Correctional |
|
Facility |
|
(If |
|
Different) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
|
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
of |
|
Birth |
|
|
|
|
|
|
|
|
‐ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Four Digits |
|
of SSN |
|
|
|
|
SBI |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E-Mail |
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing |
|
Address: |
|
Street |
|
Address/P.O. |
|
Box |
|
(include |
|
|
|
Apartment/Suite/Floor |
|
|
|
Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
Zip |
|
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Preferred Method of Communication: |
|
|
|
|
|
Mail |
|
|
|
|
|
E-Mail |
|
|
Phone |
|
|
Months (to be verified by NJDOC) |
|
Months Incarcerated at Edna Mahan Correctional |
Facility since |
January 1, |
|
2014: |
|
|
|
|
|
|
|
|
|
II. Tier Selection
Please check the box to indicate which tiered settlement you are claiming and whether you are requesting a hearing (where
applicable). For a complete description of each tier and definition of terms, please refer to the legal notice.
TIER 1 |
Compensation of $1,000 plus $20 per month (or partial month) incarcerated at Edna Mahan Correctional |
|
Facility since January 1, 2014. Selection of this tier does not require any additional documentation, with |
|
payment expected by January 27, 2022. |
Compensation of up to $4,500 for victims who experienced sexual harassment while incarcerated at Edna Mahan Correctional Facility. Selection of this tier requires a separate affidavit or certification describing the sexual harassment you claim you experienced. Claimants selecting this tier also have the option of submitting contemporaneous corroborating documentation with their claim and requesting a hearing. Payment will be made for claimants in this tier after all Tier 2 and Tier 3 claims have been heard and decided. If no selection is made below, no hearing will be requested.
YES, I would like to request a hearing for my claim
NO, I do not request a hearing for my claim
Compensation of up to $250,000 for victims who experienced sexual abuse while incarcerated at Edna Mahan Correctional Facility. Selection of this tier requires a separate affidavit or certification describing the sexual abuse you claim you experienced plus contemporaneous corroborating documentation. A hearing is mandatory for Tier 3 claims. Payments will be made for claimants in this tier after all Tier 2 and Tier 3 claims have been heard and decided.
EDNA MAHAN CORRECTIONAL FACILITY FOR WOMEN CLASS ACTION SETTLEMENT
Superior Court of New Jersey, Hunterdon County
III. Pro Bono Assistance
For Tier 2 claimants who are requesting a hearing, and Tier 3 claimants who are required to have a hearing, please indicate whether you are interested in receiving assistance from representatives of a New Jersey-based law school clinic in preparing your certification and/or affidavit, collecting supporting documentation, and preparing for your hearing.
YES, I would like assistance. Please have a clinic contact me.
NO, I would not like assistance.
IV. Certification
I certify that the above is true and correct to the best of my knowledge. I understand that if any of the foregoing is willfully false, I am
subject to punishment.
Printed Name
Reminder Checklist
1.Complete all sections of this Claim Form.
2.Sign and date the Claim Form in Section IV.
3.Keep copies of the completed Claim Form and documentation for your own records.
4.Mail your completed Claim Form to the Settlement Administrator at the address at the top of Page 1 of this Claim Form.
5.It is your responsibility to notify the Settlement Administrator of any changes to your contact information after the submission of your Claim Form. You can contact the Settlement Administrator at 1-844-810-1507 or by email at info@EMCFWsettlement.com
6.Please visit the settlement website at www.EMCFWsettlement.com for more information about this settlement.