

It is easy to complete forms with the use of our PDF editor. Updating the cms form 671 blank file is not hard for those who adhere to the following steps:
Step 1: You can press the orange "Get Form Now" button at the top of this webpage.
Step 2: Once you have accessed the editing page cms form 671 blank, you will be able to notice every one of the options readily available for the file in the upper menu.
You have to type in the next data if you want to fill out the file:
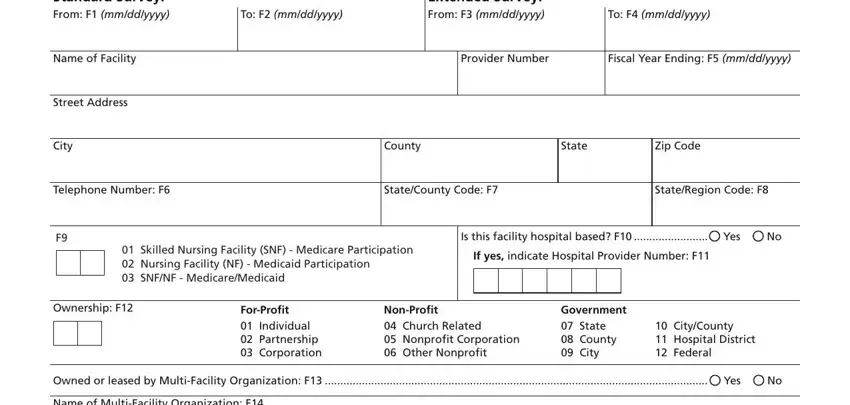
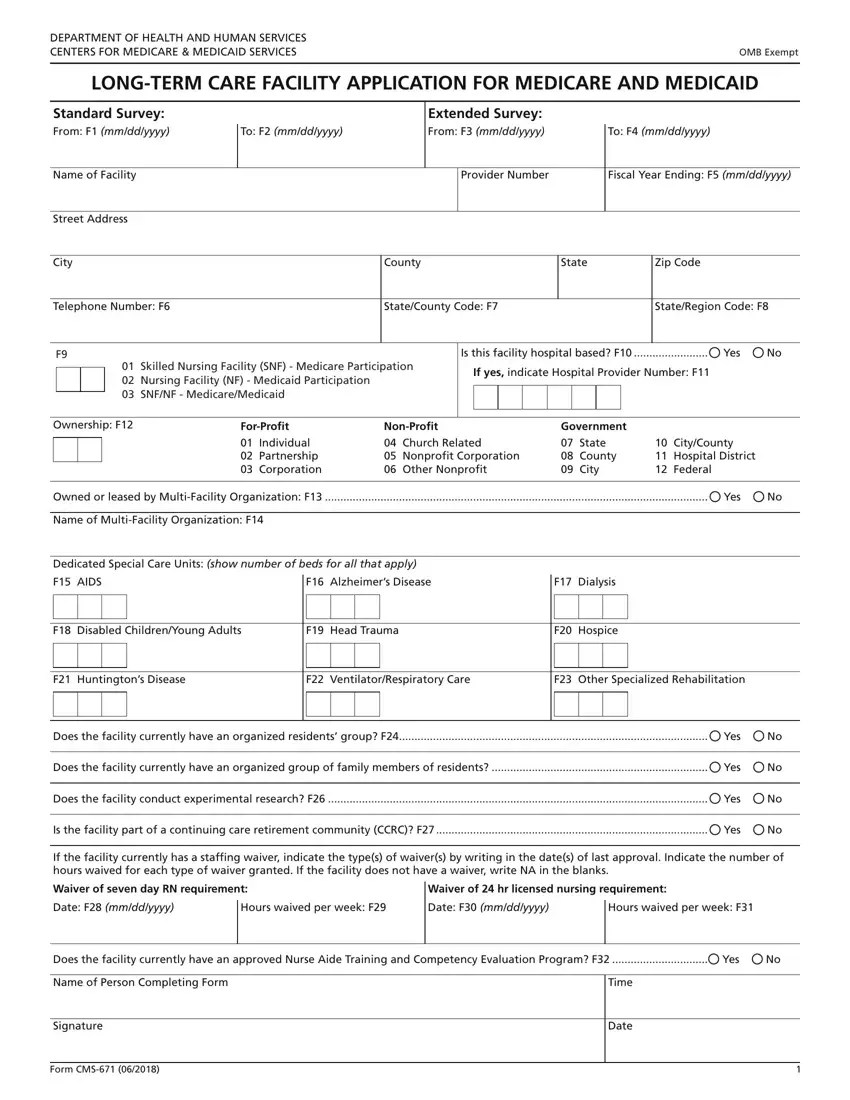
Provide the essential data in the Name of MultiFacility Organization, Dedicated Special Care Units show, F AIDS, F Alzheimers Disease, F Dialysis, F Disabled ChildrenYoung Adults, F Head Trauma, F Hospice, F Huntingtons Disease, F VentilatorRespiratory Care, F Other Specialized Rehabilitation, Does the facility currently have, Yes, Does the facility currently have, and Yes segment.
In the Waiver of seven day RN requirement, Waiver of hr licensed nursing, Date F mmddyyyy, Hours waived per week F, Date F mmddyyyy, Hours waived per week F, Does the facility currently have, Yes, Name of Person Completing Form, Signature, Form CMS, Time, and Date area, emphasize the relevant information.
Step 3: As soon as you've selected the Done button, your form should be readily available export to any gadget or email address you identify.
Step 4: Attempt to make as many copies of your file as you can to keep away from possible misunderstandings.
