You can certainly fill in forms with the help of our PDF editor. Modifying the Form Cms 847 document is straightforward if you use these actions:
Step 1: The first step would be to click on the orange "Get Form Now" button.
Step 2: At this point, you are on the file editing page. You can add text, edit existing information, highlight certain words or phrases, put crosses or checks, insert images, sign the template, erase needless fields, etc.
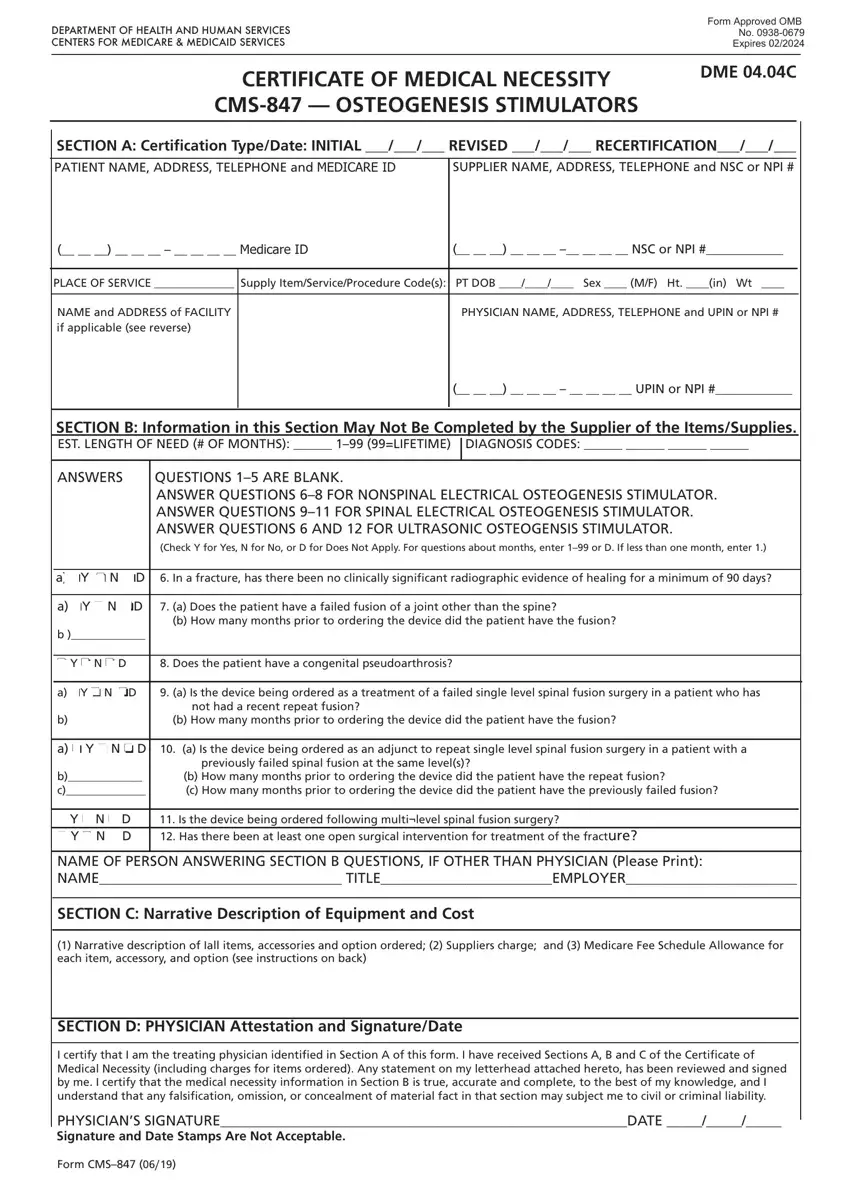
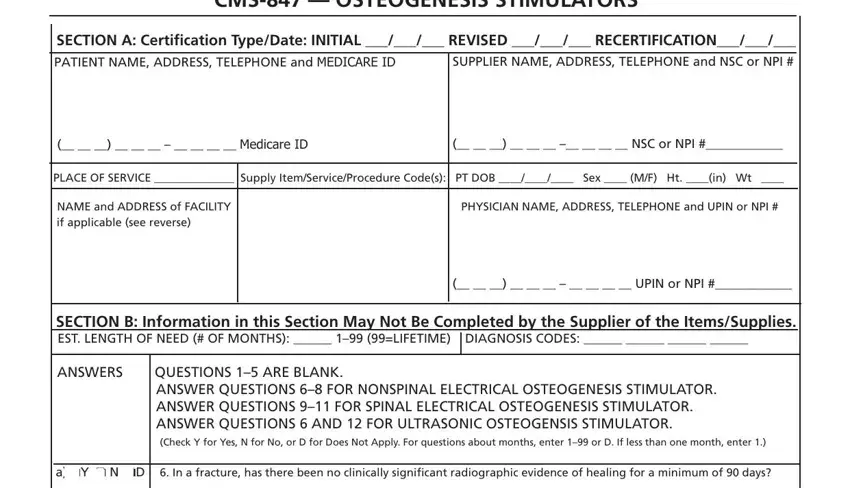
Type in the data requested by the application to fill out the file.
In the a Does the patient have a failed, How many months prior to ordering, a oY o N oD, o Y o N o, Does the patient have a, a oY o N oD, a Is the device being ordered as, b How many months prior to, a o Y o N o, D a Is the device being ordered, b c, b How many months prior to, previously failed spinal fusion at, o Y o N o D o Y o N o D, and Is the device being ordered field, note down your data.
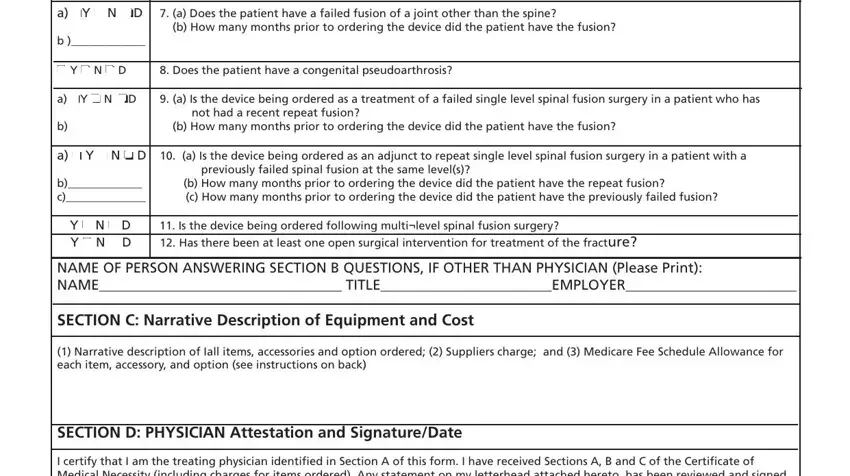
The program will require for additional info as a way to quickly prepare the section I certify that I am the treating, PHYSICIANS SIGNATUREDATE, and Form CMS.

Step 3: As you hit the Done button, your finalized document is simply transferable to any type of of your gadgets. Or alternatively, you can send it through email.
Step 4: To prevent probable forthcoming troubles, ensure that you have at the very least a few copies of any form.
