A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
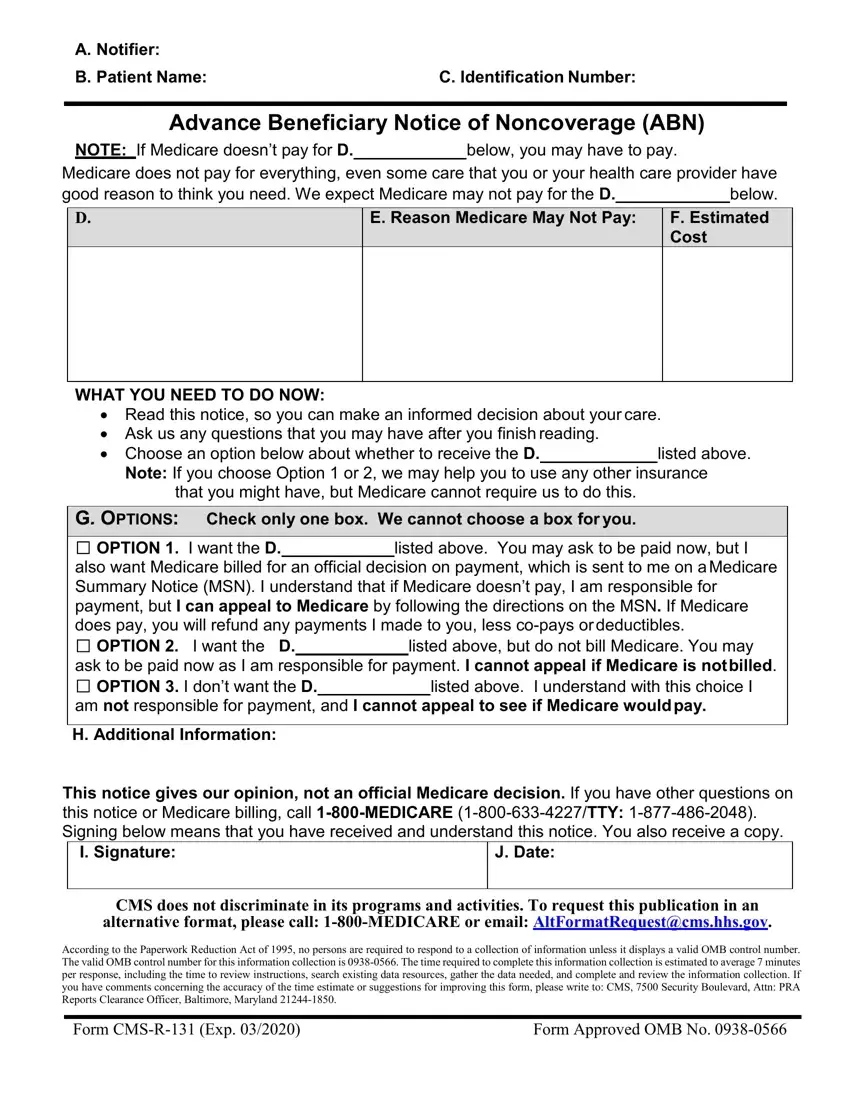
Advance Beneficiary Notice of Noncoverage (ABN)
NOTE: If Medicare doesn’t pay for D. below, you may have to pay.
Medicare does not pay for everything, even some care that you or your health care provider have
good reason to think you need. We expect Medicare may not pay for the D. |
|
below. |
E. Reason Medicare May Not Pay:
WHAT YOU NEED TO DO NOW:
•Read this notice, so you can make an informed decision about your care.
•Ask us any questions that you may have after you finish reading.
• Choose an option below about whether to receive the D.listed above.
Note: If you choose Option 1 or 2, we may help you to use any other insurance that you might have, but Medicare cannot require us to do this.
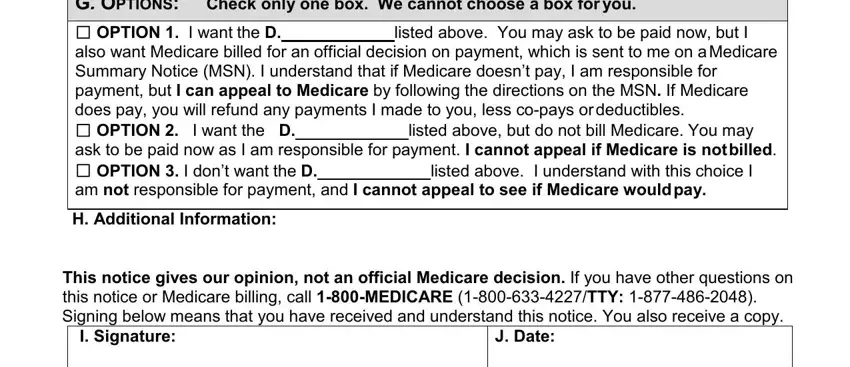
G. OPTIONS: Check only one box. We cannot choose a box for you.
□OPTION 1. I want the D. listed above. You may ask to be paid now, but I also want Medicare billed for an official decision on payment, which is sent to me on aMedicare Summary Notice (MSN). I understand that if Medicare doesn’t pay, I am responsible for payment, but I can appeal to Medicare by following the directions on the MSN. If Medicare does pay, you will refund any payments I made to you, less co-pays ordeductibles.
□ OPTION 2. I want the D. listed above, but do not bill Medicare. You may
ask to be paid now as I am responsible for payment. I cannot appeal if Medicare is notbilled.
□ OPTION 3. I don’t want the D. listed above. I understand with this choice I
am not responsible for payment, and I cannot appeal to see if Medicare wouldpay.
H. Additional Information:
This notice gives our opinion, not an official Medicare decision. If you have other questions on this notice or Medicare billing, call 1-800-MEDICARE (1-800-633-4227/TTY: 1-877-486-2048). Signing below means that you have received and understand this notice. You also receive a copy.
CMS does not discriminate in its programs and activities. To request this publication in an alternative format, please call: 1-800-MEDICARE or email: AltFormatRequest@cms.hhs.gov.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-0566. The time required to complete this information collection is estimated to average 7 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Baltimore, Maryland 21244-1850.
Form CMS-R-131 (Exp. 03/2020) |
Form Approved OMB No. 0938-0566 |
Form Instructions
Advance Beneficiary Notice of Noncoverage (ABN)
OMB Approval Number: 0938-0566
Overview
The ABN is a notice given to beneficiaries in Original Medicare to convey that Medicare is not likely to provide coverage in a specific case. “Notifiers” include physicians, providers (including institutional providers like outpatient hospitals), practitioners and suppliers paid under Part B (including independent laboratories), as well as hospice providers and religious non-medical health care institutions (RNHCIs) paid exclusively under Part A. Since 2013, home health agencies (HHAs) providing care under Part A or Part B issue the ABN instead of the Home Health Advance Beneficiary Notice (HHABN) Option Box 1 to inform beneficiaries of potential liability. The HHABN has been discontinued.
All of the aforementioned physicians, suppliers, practitioners, and providers must complete the ABN as described below, and deliver the notice to affected beneficiaries or their representative before providing the items or services that are the subject of the notice. Medicare inpatient hospitals and skilled nursing facilities (SNFs) use other approved notices for Part A items and services when notice is required; however, these facilities must use the ABN for Part B items and services.
The ABN must be reviewed with the beneficiary or his/her representative and any questions raised during that review must be answered before it is signed. The ABN must be delivered far enough in advance that the beneficiary or representative has time to consider the options and make an informed choice. Employees or subcontractors of the notifier may deliver the ABN. ABNs are never required in emergency or urgent care situations. Once all blanks are completed and the form is signed, a copy is given to the beneficiary or representative. In all cases, the notifier must retain a copy of the ABN delivered to the beneficiary on file.
The ABN may also be used to provide voluntary notification of financial liability for items or services that Medicare never covers. When the ABN is used as a voluntary notice, the beneficiary doesn’t choose an option box or sign the notice. CMS has issued detailed instructions on the use of the ABN in its on-line Medicare Claims Processing Manual (MCPM), Publication 100-04, Chapter 30, §50. Related policies on billing and coding of claims, as well as coverage determinations, are found elsewhere in the CMS manual system or website: www.cms.gov.
ABN Changes
The ABN is a formal information collection subject to approval by the Executive Office of Management and Budget (OMB) under the Paperwork Reduction Act of 1995 (PRA). As part of this process, the notice is subject to public comment and re-approval every 3 years. With the 2016 PRA submission, a non-substantive change has been made to the ABN. In accordance with Section 504 of the Rehabilitation Act of 1973 (Section 504), the form has
been revised to include language informing beneficiaries of their rights to CMS nondiscrimination practices and how to request the ABN in an alternative format if needed.
Completing the Notice
ABNs may be downloaded from the CMS website at: http://www.cms.gov/Medicare/Medicare-General-Information/BNI/ABN.html . Notices should be used as is since the ABN is a standardized OMB-approved notice. However, some allowance for customization of format is allowed as mentioned in these instructions and the on-line manual instructions for those choosing to integrate the ABN into other automated business processes. Instructions for completion of the form are set forth below:
ABNs must be reproduced on a single page. The page may be either letter or legal-size, with additional space allowed for each blank needing completion when a legal-size page is used.
Sections and Blanks:
There are 10 blanks for completion in this notice, labeled from (A) through (J), with accompanying instructions for each blank below. We recommend that notifiers remove the lettering labels from the blanks before issuing the ABN to beneficiaries. Blanks (A)-(F) and blank (H) may be completed prior to delivering the notice, as appropriate. Entries in the blanks may be typed or hand-written, but should be large enough (i.e., approximately 12-point font) to allow ease in reading. (Note that 10 point font can be used in blanks when detailed information must be given and is otherwise difficult to fit in the allowed space.) The notifier must also insert the blank (D) header information into all of the blanks labeled (D) within the Option Box section, Blank (G). One of the check boxes in the Option Box section, Blank (G), must be selected by the beneficiary or his/her representative. Blank (I) should be a cursive signature, with printed annotation if needed in order to be understood.
Header
Blanks A-C, the header of the notice, must be completed by the notifier prior to delivering the ABN.
Blank (A) Notifier(s): Notifiers must place their name, address, and telephone number (including TTY number when needed) at the top of the notice. This information may be incorporated into a notifier’s logo at the top of the notice by typing, hand-writing, pre- printing, using a label or other means.
If the billing and notifying entities are not the same, the name of more than one entity may be given in the Header as long as it is specified in the Additional Information (H) section who should be contacted for billing questions.
Blank (B) Patient Name: Notifiers must enter the first and last name of the beneficiary receiving the notice, and a middle initial should also be used if there is one on the beneficiary’s Medicare (HICN) card. The ABN will not be invalidated by a misspelling or missing initial, as long as the beneficiary or representative recognizes the name listed on the notice as that of the beneficiary.
Blank (C) Identification Number: Use of this field is optional. Notifiers may enter an identification number for the beneficiary that helps to link the notice with a related claim. The absence of an identification number does not invalidate the ABN. An internal filing number created by the notifier, such as a medical record number, may be used. Medicare numbers (HICNs) or Social Security numbers must not appear on the notice.
Body
Blank (D): The following descriptors may be used in the Blank (D) fields:
Item
Service
Laboratory test
Test
Procedure
Care
Equipment
The notifier must list the specific names of the items or services believed to be noncovered in the column directly under the header of Blank (D).
In the case of partial denials, notifiers must list in the column under Blank (D) the excess component(s) of the item or service for which denial is expected.
For repetitive or continuous noncovered care, notifiers must specify the frequency and/or duration of the item or service. See § 50.7.1 (b) of the MCPM, Chapter 30 for additional information.
General descriptions of specifically grouped supplies are permitted in this column. For example, “wound care supplies” would be a sufficient description of a group of items used to provide this care. An itemized list of each supply is generally not required.
When a reduction in service occurs, notifiers must provide enough additional information so that the beneficiary understands the nature of the reduction. For example, entering “wound care supplies decreased from weekly to monthly” would be appropriate to describe a decrease in frequency for this category of supplies; just writing “wound care supplies decreased” is insufficient.
Please note that there are a total of 7 Blank (D) fields that the notifier must complete on the ABN. Notifiers are encouraged to populate all of the Blank (D) fields in advance when a general descriptor such as “Item(s)/Service(s)” is used. All Blank
(D)fields must be completed on the ABN in order for the notice to be considered valid.
Blank (E) Reason Medicare May Not Pay: In the column under this header, notifiers must explain, in beneficiary friendly language, why they believe the items or services listed in the column under Blank (D) may not be covered by Medicare. Three commonly used reasons for noncoverage are:
“Medicare does not pay for this test for your condition.”
“Medicare does not pay for this test as often as this (denied as too frequent).”
“Medicare does not pay for experimental or research use tests.”
To be a valid ABN, there must be at least one reason applicable to each item or service listed in the column under Blank (D). The same reason for noncoverage may be applied to multiple items in Blank (D) when appropriate.
Blank (F) Estimated Cost: Notifiers must complete the column under Blank (F) to ensure the beneficiary has all available information to make an informed decision about whether or not to obtain potentially noncovered services.
Notifiers must make a good faith effort to insert a reasonable estimate for all of the items or services listed under Blank (D). In general, we would expect that the estimate should be within $100 or 25% of the actual costs, whichever is greater; however, an estimate that exceeds the actual cost substantially would generally still be acceptable, since the beneficiary would not be harmed if the actual costs were less than predicted. Thus, examples of acceptable estimates would include, but not be limited to, the following:
For a service that costs $250:
•Any dollar estimate equal to or greater than $150
•“Between $150-300”
•“No more than $500”
For a service that costs $500:
•Any dollar estimate equal to or greater than $375
•“Between $400-600”
•“No more than $700”
Multiple items or services that are routinely grouped can be bundled into a single cost estimate. For example, a single cost estimate can be given for a group of laboratory tests, such as a basic metabolic panel (BMP). An average daily cost estimate is also permissible for long term or complex projections. As noted above, providers may also pre-print a menu of items or services in the column under Blank (D) and include a cost estimate alongside each item or service. If a situation involves the possibility of additional tests or procedures (such as in laboratory reflex testing), and the costs associated with such tests cannot be reasonably estimated by the notifier at the time of ABN delivery, the notifier may enter the initial cost estimate and indicate the possibility of further testing. Finally, if for some reason the notifier is unable to provide a good faith estimate of projected costs at the time of ABN delivery, the notifier may indicate in the cost estimate area that no cost estimate is available. We would not expect either of these last two scenarios to be routine or frequent practices,but the beneficiary would have the option of signing the ABN and accepting liability in these situations.
CMS will work with its contractors to ensure consistency when evaluating cost estimatesand determining validity of the ABN in general. In addition, contractors will provide ongoing education to notifiers as needed to ensure proper notice delivery. Notifiers should contact the appropriate CMS regional office if they believe that a contractor inappropriately invalidated an ABN.
Options
Blank (G) Options: Blank (G) contains the following three options:
□OPTION 1. I want the (D) listed above. You may ask to be paid now, but I also want Medicare billed for an official decision on payment, which is sent to me on a Medicare Summary Notice (MSN). I understand that if Medicare doesn’t pay, I am responsible for payment, but I can appeal to Medicare by following the directions on the MSN. If Medicare does pay, you will refund any payments I made to you, less co-pays ordeductibles.
This option allows the beneficiary to receive the items and/or services at issue and requires the notifier to submit a claim to Medicare. This will result in a payment decision that can be appealed. See Ch. 30, §50.15.1 of the online Medicare Claims Processing Manual for instructions on the notifier’s obligation to bill Medicare. Suppliers and providers who don’t accept Medicare assignment may make modifications to Option 1 only as specified below under “D. Additional Information.”
Note: Beneficiaries who need to obtain an official Medicare decision in order to file a claim with a secondary insurance should choose Option 1.
□OPTION 2. I want the (D) listed above, but do not bill Medicare. You may ask to be paid now as I am responsible for payment. I cannot appeal if Medicare isnot billed.
This option allows the beneficiary to receive the noncovered items and/or services and pay for them out of pocket. No claim will be filed and Medicare will not be billed. Thus, there are no appeal rights associated with this option.
□OPTION 3. I don’t want the (D)listed above. I understand with this choice I am not responsible for payment, and I cannot appeal to see if Medicare wouldpay.
This option means the beneficiary does not want the care in question. By checking this box, the beneficiary understands that no additional care will be provided; thus, there are no appeal rights associated with this option.
The beneficiary or his or her representative must choose only one of the three options listed in Blank (G). Under no circumstances can the notifier decide for the beneficiary which of the 3 checkboxes to select. Pre-selection of an option by the notifier invalidates the notice. However, at the beneficiary’s request, notifiers may enter the beneficiary’s selection if he or she is physically unable to do so. In such cases, notifiers must annotate the notice accordingly.
If there are multiple items or services listed in Blank (D) and the beneficiary wants to receive some, but not all of the items or services, the notifier can accommodate this request by using more than one ABN. The notifier can furnish an additional ABN listing the items/services the beneficiary wishes to receive with the corresponding option.
If the beneficiary cannot or will not make a choice, the notice should be annotated, for
example: “beneficiary refused to choose an option.”
Additional Information
Blank (H) Additional Information: Notifiers may use this space to provide additional clarification that they believe will be of use to beneficiaries. For example, notifiers may use this space to include:
A statement advising the beneficiary to notify his or her provider about certain tests that were ordered, but not received;
Information on other insurance coverage for beneficiaries, such as a Medigap policy, if applicable;
An additional dated witness signature; or Other necessary annotations.
Annotations will be assumed to have been made on the same date as that appearing in Blank J, accompanying the signature. If annotations are made on different dates, those dates should be part of the annotations.
Special guidance ONLY for non-participating suppliers and providers (those who don’t accept Medicare assignment):
Strike the last sentence in the Option 1 paragraph with a single line so that it appears like this: If Medicare does pay, you will refund any payments I made to you, less co- pays or deductibles.
This single line strike can be included on ABNs printed specifically for issuance when unassigned items and services are furnished. Alternatively, the line can be hand-penned on an already printed ABN.
The sentence must be stricken and can’t be entirely concealed or deleted.
There is no CMS requirement for suppliers or the beneficiary to place initials next to the stricken sentence or date the annotations when the notifier makes the changes to the ABN before issuing the notice to the beneficiary.
When this sentence is stricken, the supplier shall include the following CMS-approved unassigned claim statement in the (H) Additional Information section.
“This supplier doesn’t accept payment from Medicare for the item(s) listed in the table above. If I checked Option 1 above, I am responsible for paying the supplier’s charge for the item(s) directly to the supplier. If Medicare does pay, Medicare will pay me the Medicare-approved amount for the item(s), and this payment to me may be less than the supplier’s charge.”
OThis statement can be included on ABNs printed for unassigned items and services, or it can be handwritten in a legible 10 point or larger font.
•An ABN with the Option 1 sentence stricken must contain the CMS-approved unassigned claim statement as written above to be considered valid notice. Similarly, when the unassigned claim statement is included in the “Additional Information” section, the last sentence in Option 1 should be stricken.
B. Signature Box
Once the beneficiary reviews and understands the information contained in the ABN, the Signature Box is to be completed by the beneficiary (or representative). This box cannot be completed in advance of the rest of the notice.
Blank (I) Signature: The beneficiary (or representative) must sign the notice to indicate that he or she has received the notice and understands its contents. If a representative signs on behalf of a beneficiary, he or she should write out “representative” in parentheses after his or her signature. The representative’s name should be clearly legible or noted in print.
Blank (J) Date: The beneficiary (or representative) must write the date he or she signed the ABN. If the beneficiary has physical difficulty with writing and requests assistance in completing this blank, the date may be inserted by the notifier.
Disclosure Statement: The disclosure statements in the footer of the notice are required to be included on the document.