It is easy to complete this form online using our PDF editor. Follow these steps to fill it out and submit it correctly:
Step 1: Click the orange "Get Form Now" button on this page to open the document in our online editor.
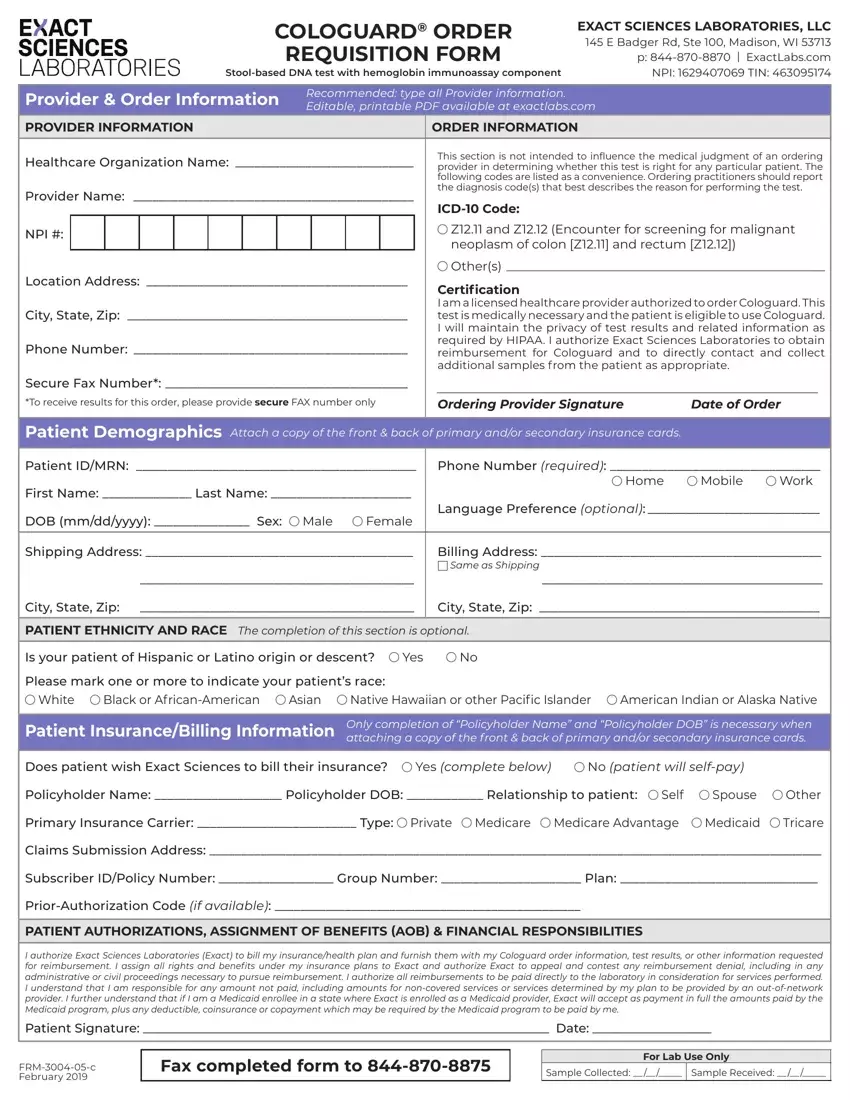
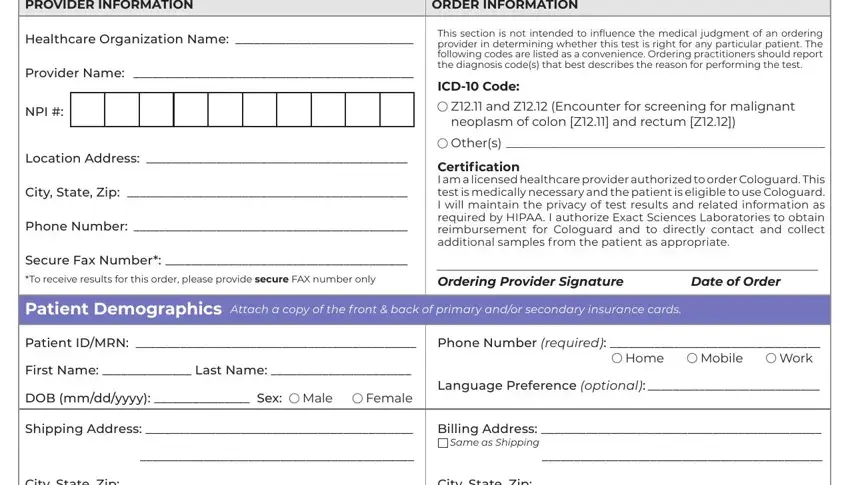
Step 2: Review all sections before entering information. The document contains provider information fields (NPI, fax number, organization name), patient demographic fields (name, date of birth, address), diagnostic code fields, and billing details. Use the toolbar to type in each field, add checkmarks, highlight text, and make other changes as needed.
Complete the provider and order information fields first, then move to the patient sections:
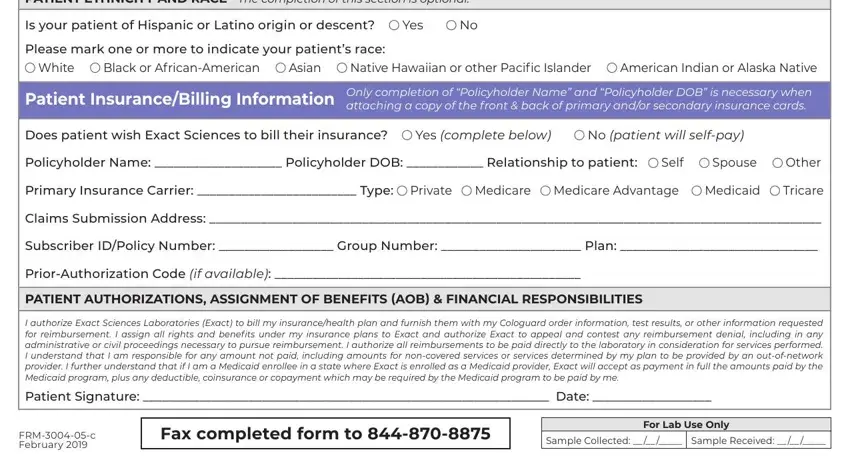
Fill in the PATIENT ETHNICITY AND RACE The, Is your patient of Hispanic or, Yes, Please mark one or more to, White, Black or AfricanAmerican, Asian, Native Hawaiian or other Pacific, American Indian or Alaska Native, Patient InsuranceBilling, Only completion of Policyholder, Does patient wish Exact Sciences, Yes complete below, No patient will selfpay, and Policyholder Name Policyholder areas with any data that will be requested by the program.
Step 3: Click the "Done" button when you have completed all required fields. Download the PDF to your device or send it by fax to Exact Sciences.
Step 4: Save a copy of the completed document for your records. Your information is kept confidential.
Frequently asked questions about this form
What information do providers need before filling out this requisition?
Have the following ready before starting: the ordering provider's NPI number and office fax number, the patient's full name and date of birth, the patient's insurance ID and group number, and the appropriate ICD-10 diagnostic code. The most commonly used code is Z12.11 for colorectal cancer screening.
Can this requisition be submitted electronically?
Yes. After completing the form online, download the PDF and submit it by fax to Exact Sciences at the number printed on the form. Electronic submission is also available for practices registered with EpicCare Link. Call 1-844-870-8870 for ordering assistance.
Who is eligible for the Cologuard colorectal cancer screening test?
The test is for adults aged 45 and older who are at average risk for colorectal cancer. Average risk means no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease. The ordering provider certifies patient eligibility in the certification section.
What is the difference between the order form and the requisition form?
The terms "cologuard order form" and "cologuard order requisition form" refer to the same document. Both names describe the PDF that healthcare providers use to request the Cologuard colorectal cancer screening test from Exact Sciences Laboratories.
For related medical ordering documents, browse the internal requisition form and the lab requisition form pages.
