
How to Complete the NC Communicable Disease Report Form
The North Carolina Communicable Disease Report form must be submitted to your local health department as soon as a reportable disease or condition is diagnosed or suspected. Healthcare providers, hospitals, laboratories, and schools are all required reporters under NC state law. Use this guide to complete the form accurately and avoid processing delays.
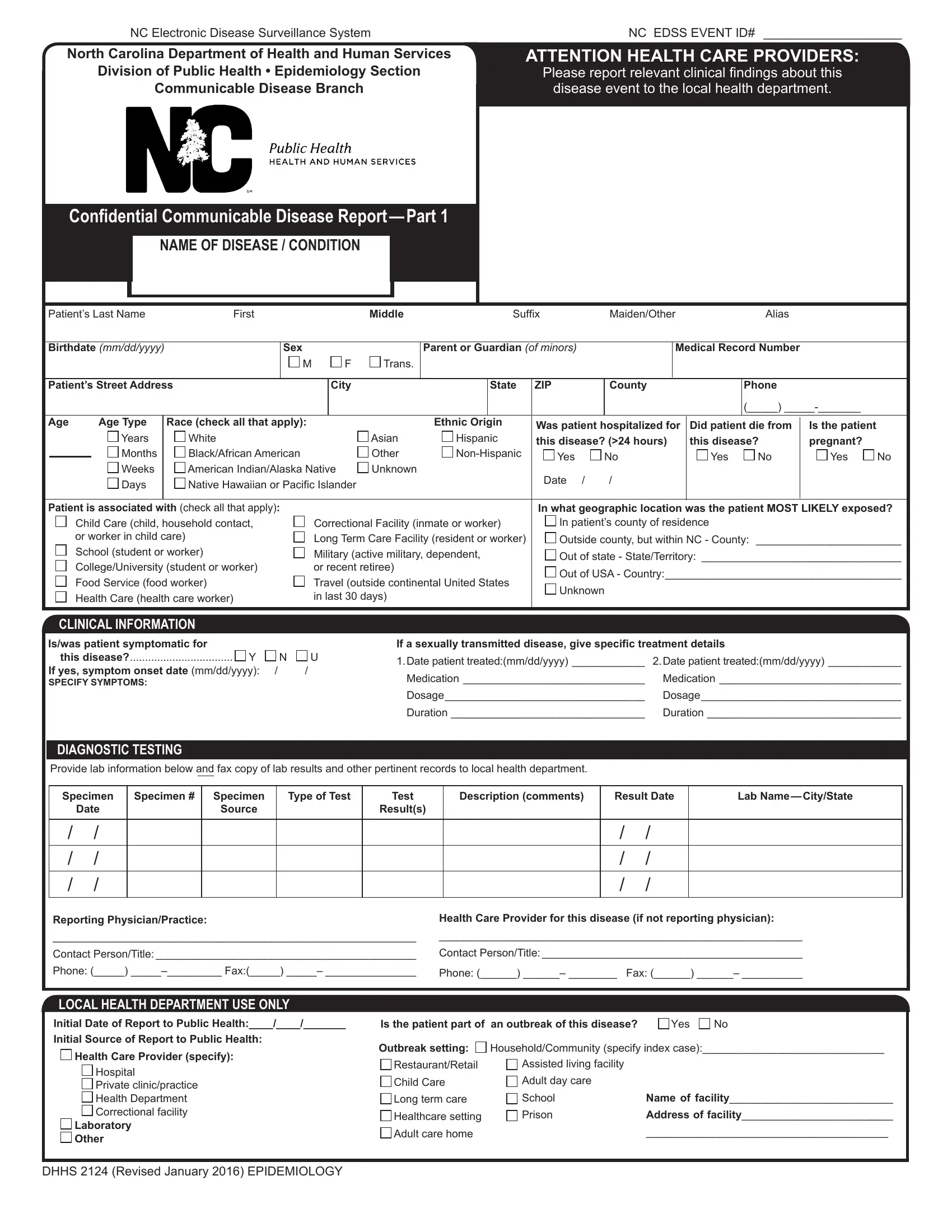
Required Information for Each Section
Gather the following details before starting the form:
- Patient identification: Full legal name, date of birth, current address, sex, race, and ethnicity.
- Disease or condition: Reportable disease name, date of symptom onset, and current clinical status.
- Clinical findings: Primary symptoms, physical examination results, and relevant medical history.
- Laboratory results: Test type, specimen collection date, laboratory name, and test result.
- Exposure details: Potential exposure sources, travel history within the relevant incubation period, and known contacts.
- Reporting provider: Provider name, facility name, phone number, address, and date of report.
Confidentiality and Privacy Requirements
All information submitted on the communicable disease report is confidential. Under NC General Statute 130A-143, disease report data is exempt from public records disclosure requirements and protected from unauthorized use. Patient information is used exclusively for public health investigation, disease surveillance, and coordinated response efforts by local and state health agencies.
Related Medical and Health Forms
You may also need these related forms when managing patient health documentation:
- Medical Report Form for documenting general clinical findings
- Physician Medical Report Form for physician-completed clinical assessments
- BSA Health Form for health history and physical examination records
- North Carolina DNR Form for do-not-resuscitate documentation