
Completing the asonet dental file is easy using our PDF editor. Keep up with the following steps to get the document ready without delay.
Step 1: Select the orange button "Get Form Here" on the page.
Step 2: The form editing page is currently open. You can include text or update current data.
Make sure you provide the next information to complete the asonet dental PDF:
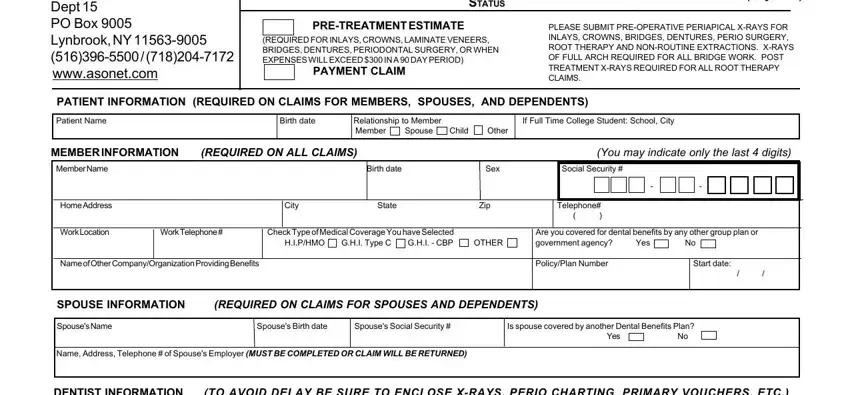
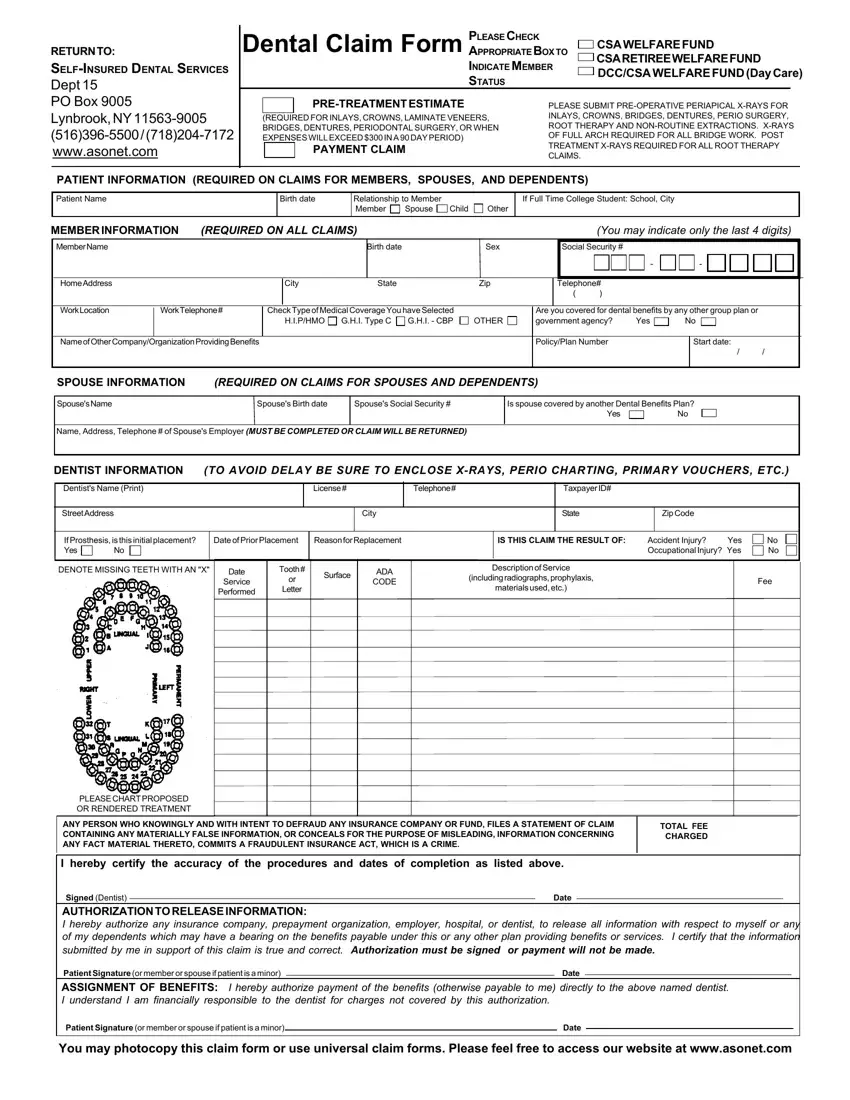
Fill out the DENTIST INFORMATION, TO AVOID DELAY BE SURE TO ENCLOSE, Dentists Name Print, License, Telephone, Taxpayer ID, Street Address, City, State, Zip Code, If Prosthesis is this initial, DENOTE MISSING TEETH WITH AN X, Date of Prior Placement, Reason for Replacement, and IS THIS CLAIM THE RESULT OF fields with any particulars which may be asked by the system.
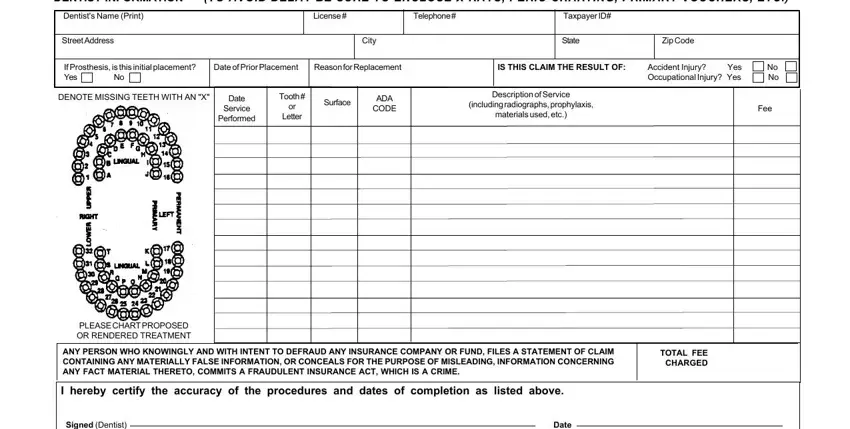
You may be requested to type in the particulars to help the program prepare the section Signed Dentist AUTHORIZATION TO, Patient Signature or member or, Date, Patient Signature or member or, Date, and You may photocopy this claim form.

Step 3: Select "Done". You can now upload the PDF document.
Step 4: Ensure you prevent upcoming difficulties by having minimally 2 copies of the file.
