

ged transcripts can be filled out online effortlessly. Just open FormsPal PDF editing tool to perform the job promptly. To make our editor better and more convenient to utilize, we consistently work on new features, with our users' suggestions in mind. Getting underway is simple! All you should do is stick to the next simple steps down below:
Step 1: Access the PDF form inside our editor by clicking on the "Get Form Button" at the top of this page.
Step 2: As you access the editor, you will get the document all set to be filled in. Other than filling out various fields, it's also possible to perform many other things with the Document, specifically putting on your own textual content, modifying the initial textual content, inserting graphics, affixing your signature to the document, and much more.
As for the blank fields of this particular document, here is what you want to do:
1. You should fill out the ged transcripts correctly, thus pay close attention when filling in the sections comprising these specific blank fields:
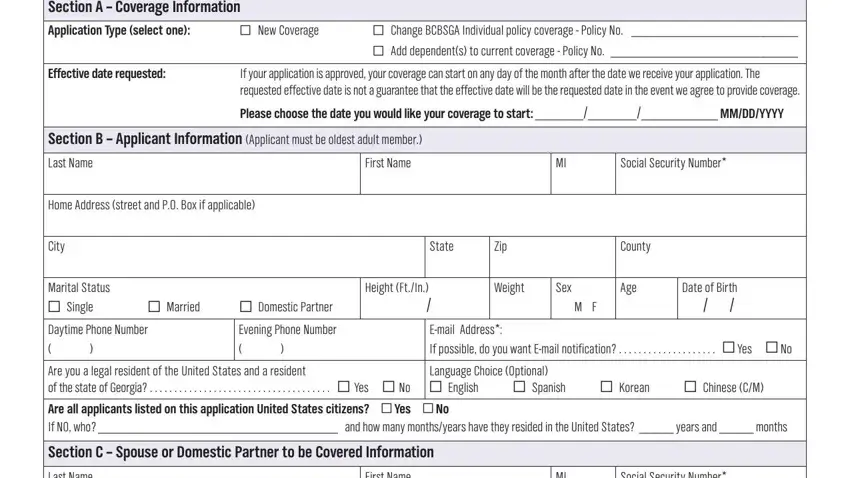
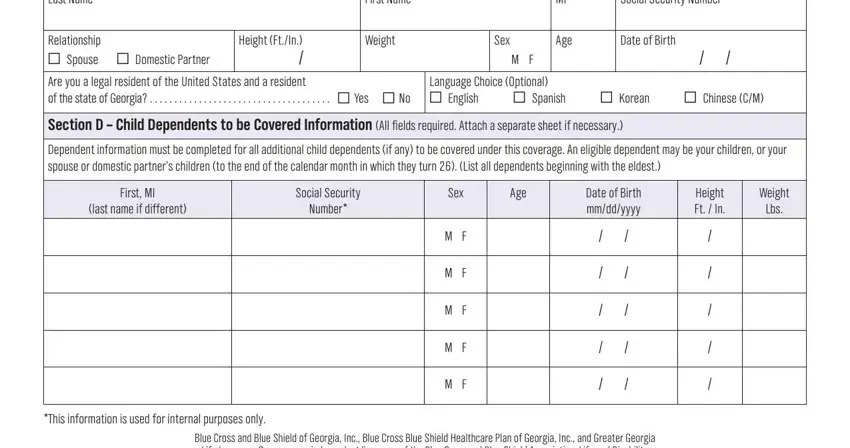
2. Once this section is finished, you need to add the essential details in Last Name, First Name, Relationship Spouse Domestic, Height FtIn Are you a legal, Weight, Age, Sex, M F, Social Security Number, Date of Birth, Language Choice Optional English, Spanish, Korean, Chinese CM, and Section D Child Dependents to be in order to progress further.
3. The following step is related to BCBSGA will enroll all eligible, I the Applicant request that, Premier Plus POS, EQ ER, Consumer Choice Option, Maternity Rider, Premier Plus PPO, Consumer Choice Option, Maternity Rider, SmartSense Plus POS, FG FH, Consumer Choice Option, Enhanced Drug Rider, SmartSense Plus PP, and EY EZ - type in these blanks.
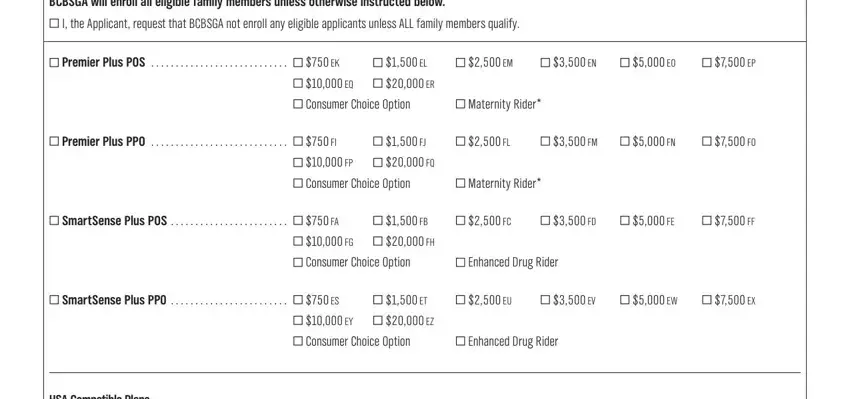
People who work with this document generally make errors while completing Consumer Choice Option in this part. Ensure you read twice what you type in right here.
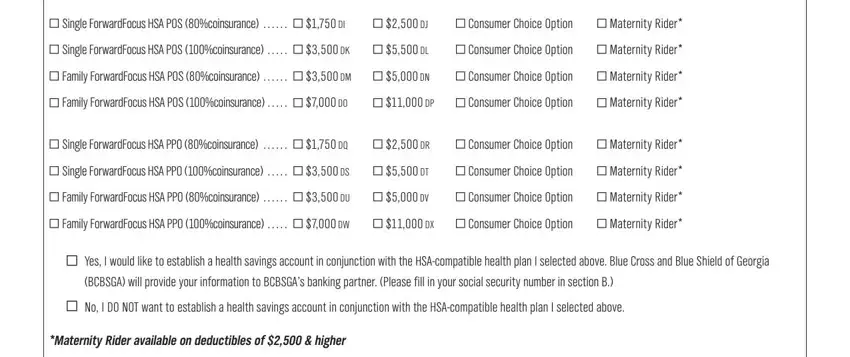
4. To go onward, the next stage requires filling in several form blanks. Examples of these are Single ForwardFocus HSA POS, Consumer Choice Option, Maternity Rider, Single ForwardFocus HSA POS, Consumer Choice Option, Maternity Rider, Family ForwardFocus HSA POS, Consumer Choice Option, Maternity Rider, Family ForwardFocus HSA POS, Consumer Choice Option, Maternity Rider, Single ForwardFocus HSA PPO, Consumer Choice Option, and Maternity Rider, which you'll find integral to moving forward with this PDF.
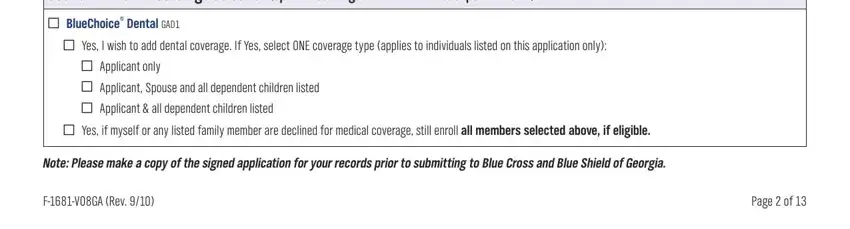
5. This form needs to be wrapped up by dealing with this area. Below one can find an extensive set of blank fields that need specific information in order for your document usage to be accomplished: Section F Dental Coverage, BlueChoice Dental GAD, Yes I wish to add dental coverage, Applicant only, Applicant Spouse and all, Applicant all dependent children, Yes if myself or any listed, Note Please make a copy of the, FVGA Rev, and Page of.
Step 3: After double-checking the fields and details, press "Done" and you are good to go! Obtain your ged transcripts the instant you register at FormsPal for a free trial. Easily access the pdf document within your FormsPal account, along with any edits and changes being all preserved! Here at FormsPal, we strive to make sure that all your details are maintained private.