STATE OF NEW YORK
WORKERS' COMPENSATION BOARD
DISABILITY BENEFITS BUREAU
100BROADWAY-MENANDS ALBANY, NY. 12241 - 0005
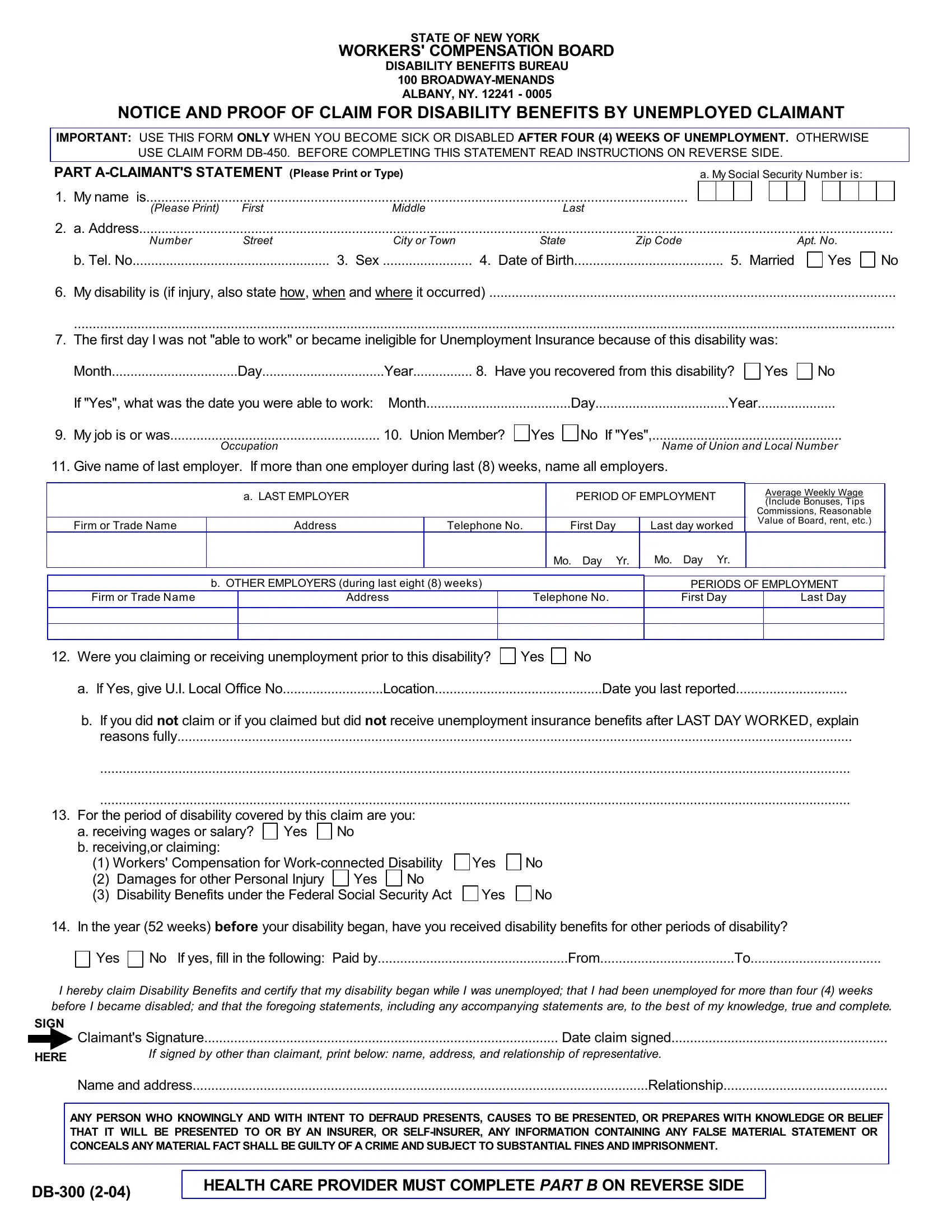
NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS BY UNEMPLOYED CLAIMANT
IMPORTANT: USE THIS FORM ONLY WHEN YOU BECOME SICK OR DISABLED AFTER FOUR (4) WEEKS OF UNEMPLOYMENT. OTHERWISE
USE CLAIM FORM DB-450. BEFORE COMPLETING THIS STATEMENT READ INSTRUCTIONS ON REVERSE SIDE.
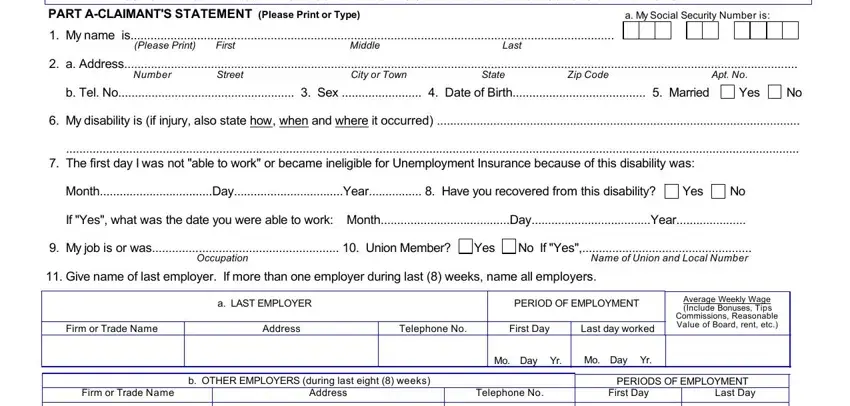
PART A-CLAIMANT'S STATEMENT (Please Print or Type) |
|
|
a. My Social Security Number is: |
|
|
1. |
My name is |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Please Print) |
First |
Middle |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
a. Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number |
Street |
City or Town |
State |
Zip Code |
|
|
|
|
|
|
Apt. No. |
|
|
|
b. Tel. No |
3. Sex |
4. Date of Birth |
|
5. Married |
|
|
Yes |
No |
6.My disability is (if injury, also state how, when and where it occurred) .............................................................................................................
............................................................................................................................................................................................................................
7.The first day I was not "able to work" or became ineligible for Unemployment Insurance because of this disability was:
|
|
|
|
|
|
|
Month |
Day |
Year |
8. Have you recovered from this disability? |
Yes |
No |
If "Yes", what was the date you were able to work: |
Month |
Day |
Year |
|
9. My job is or was |
10. Union Member? |
|
Occupation |
No If "Yes",...................................................
Name of Union and Local Number
11. Give name of last employer. If more than one employer during last (8) weeks, name all employers.
|
a. LAST EMPLOYER |
|
PERIOD OF EMPLOYMENT |
|
Average Weekly Wage |
|
|
|
(Include Bonuses, Tips |
|
|
|
|
|
|
Commissions, Reasonable |
Firm or Trade Name |
Address |
Telephone No. |
First Day |
Last day worked |
Value of Board, rent, etc.) |
|
|
|
|
Mo. Day Yr. |
Mo. Day |
Yr. |
|
|
b. OTHER EMPLOYERS (during last eight (8) weeks) |
Firm or Trade Name |
|
Address |
|
|
|
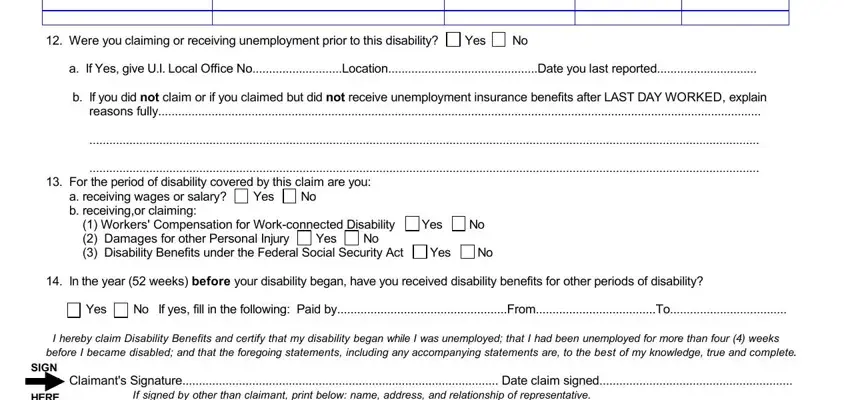
12. Were you claiming or receiving unemployment prior to this disability? Yes No
a. If Yes, give U.I. Local Office No |
Location |
Date you last reported |
b.If you did not claim or if you claimed but did not receive unemployment insurance benefits after LAST DAY WORKED, explain reasons fully.....................................................................................................................................................................................
.........................................................................................................................................................................................................
.........................................................................................................................................................................................................
13.For the period of disability covered by this claim are you:
a. receiving wages or salary? |
Yes |
No |
|
|
|
|
b. receiving,or claiming: |
|
|
|
|
|
|
(1) Workers' Compensation for Work-connected Disability |
|
Yes |
|
No |
(2)Damages for other Personal Injury Yes No
(3)Disability Benefits under the Federal Social Security Act Yes No
14.In the year (52 weeks) before your disability began, have you received disability benefits for other periods of disability?
Yes |
No If yes, fill in the following: Paid by |
From |
To |
I hereby claim Disability Benefits and certify that my disability began while I was unemployed; that I had been unemployed for more than four (4) weeks before I became disabled; and that the foregoing statements, including any accompanying statements are, to the best of my knowledge, true and complete.
SIGN
|
|
Claimant's Signature |
Date claim signed |
|
|
HERE |
If signed by other than claimant, print below: name, address, and relationship of representative. |
|
|
Name and address |
Relationship |
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD PRESENTS, CAUSES TO BE PRESENTED, OR PREPARES WITH KNOWLEDGE OR BELIEF THAT IT WILL BE PRESENTED TO OR BY AN INSURER, OR SELF-INSURER, ANY INFORMATION CONTAINING ANY FALSE MATERIAL STATEMENT OR CONCEALS ANY MATERIAL FACT SHALL BE GUILTY OF A CRIME AND SUBJECT TO SUBSTANTIAL FINES AND IMPRISONMENT.
HEALTH CARE PROVIDER MUST COMPLETE PART B ON REVERSE SIDE
PART B - HEALTH CARE PROVIDER'S STATEMENT (Please Print or Type)
THE HEALTH CARE PROVIDER'S STATEMENT MUST BE FILLED IN COMPLETELY. THE ATTENDING HEALTH CARE PROVIDER SHALL COMPLETE AND MAIL SUCH FORM TO THE WORKERS' COMPENSATION BOARD (SEE ADDRESS BELOW), OR RETURN IT TO THE CLAIMANT, WITHIN SEVEN (7) DAYS OF RECEIPT OF THIS FORM. For item 7-d, give approximate date. Make some estimate. If disability is caused by or arising in connection with pregnancy, enter estimated delivery date under "Remarks."
INCOMPLETE ANSWERS MAY DELAY PAYMENT OF BENEFITS.
1. Claimant's Name |
Middle Initial |
2. Date of Birth |
3. Sex |
First |
Last |
|
4.Diagnosis/Analysis:......................................................................................................................................................................................................
a.Claimant's symptoms:.............................................................................................................................................................................................
.................................................................................................................................................................................................................................
.................................................................................................................................................................................................................................
b.Objective findings:....................................................................................................................................................................................................
.................................................................................................................................................................................................................................
5. |
Claimant hospitalized? |
Yes |
No |
From |
To |
|
|
|
|
|
|
6. |
Operation indicated? |
Yes |
No |
a. Type |
b. Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
ENTER DATES FOR THE FOLLOWING |
|
MONTH |
DAY |
|
YEAR |
|
|
|
|
|
a. Date of your first treatment for this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Date of your most recent treatment for this disability |
|
|
|
|
|
|
|
|
|
|
c. Date Claimant was unable to work because of this disability |
|
|
|
|
|
|
|
|
|
|
d. Date Claimant will again be able to perform work |
(Even if considerable question |
|
|
|
|
|
|
|
|
|
|
exists, estimate date. Avoid use of terms such as unknown or undetermined.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
In your opinion, is this disability the result of injury arising out of and in the course of employment or occupational disease? |
|
|
|
|
|
Yes |
No If "Yes", has Form C-4 been filed with the Board? |
Yes |
No |
|
|
|
|
|
|
|
Remarks: |
|
|
|
|
|
|
|
|
|
|
|
|
.......................................................................................................................................................................................................................... |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
I affirm that I am a |
|
|
|
Licensed or |
|
License |
|
|
|
|
|
Certified in the State of |
No.: |
|
|
|
|
|
|
(Physician, Chiropractor, Dentist, Nurse-Midwife, Podiatrist or Psychologist) |
|
|
|
|
|
|
|
|
|
Health Care Provider's Printed Name |
.......................................................................... |
|
|
Signature |
Date |
|
|
|
|
|
Office |
|
|
|
|
|
Tel No |
|
|
|
|
|
Address |
Number |
Street |
|
City/town |
State |
Zip |
Signed |
|
|
|
|
|
|
|
|
|
|
|
|
|
CLAIMANT: READ THESE INSTRUCTIONS CAREFULLY - ANSWER ALL QUESTIONS
1. MAKE SURE YOU FILE THE CORRECT CLAIM FORM. This is the correct claim form to use if you become sick or disabled more than four (4) weeks AFTER you last worked.
2. COMPLETED CLAIM FOR DISABILITY BENEFITS. You complete and sign, Part A - Claimant's Statement. (If you are not able to sign
the Claimant's Statement, your representative may sign on your behalf. Place for signing is indicated by on reverse side. Your Health Care Provider completes and signs Part B - Health Care Provider's Statement.
3. FILE YOUR CLAIM FOR DISABILITY BENEFITS PROMPTLY. Your completed claim should be filed (mailed) not later than thirty (30) days after you become sick or disabled. If it is being filed late (more than 30 days after your disability began) attach a statement explaining why you could not file this claim earlier. Make a photocopy of this completed form for your records before you submit it.
Mail this form to:
Workers' Compensation Board
Disability Benefits Bureau
100 Broadway - Menands
Albany, NY, 12241-0005
Notification Pursuant to the New York Personal Privacy Protection Law (Public Officers Law Article 6-A) and the Federal Privacy Act of 1974 (5 U.S.C. Sec. 552a).
The Workers’ Compensation Board’s (“Board”) authority to request personal information from claimants is derived from Sections 20 and 142 of the Workers’ Compensation Law. This information is collected to assist the Board in processing claims in an efficient manner and to help it maintain accurate claim records.
The Board is strongly committed to protecting the confidentiality of all personal information that it collects. Such information will be disclosed within the agency only to Board personnel and agents in furtherance of their official duties. Personal information will be disclosed outside the agency only in accordance with applicable state and federal law.
The Board’s Director of Operations, located at 100 Broadway, Menands, New York 12241 (518-474-6674), is primarily responsible for the maintenance of agency records containing personal claimant information.
Failure to provide the information requested on this form will not result in the denial of your claim, but may delay the processing of your claim. The voluntary release of your social security number enables the Board to ensure that information is associated with, and quick action is taken on, your claim.
HIPAA NOTICE - In order to adjudicate a workers' compensation claim, WCL13-a(4)(a) and 12 NYCRR 325-1.3 require health care providers to regularly file medical reports of treatment with the Board and the carrier or employer. Pursuant to 45 CFR 164.512 these legally required medical reports are exempt from HIPAA's restrictions on disclosure of health information.
Disclosure of Information: The Board will not disclose any information about your case to any unauthorized party without your consent. If you choose to have such information disclosed to an unauthorized party, you must file with the Board an original signed Form OC-110A, Claimant's Authorization to Disclose Workers' Compensation Records, or an original signed, notarized authorization letter. You may telephone your local WCB office to have Form OC-110A sent to you, or you may download it from our web page, www.wcb.ny.gov. It can be found under the heading Common Forms Online. Mail the completed authorization form or letter to the address given on the front of this form.
|
IF YOU HAVE ANY QUESTIONS ABOUT CLAIMING DISABILITY BENEFITS, |
SI TIENE DUDAS RELACIONADAS CON LA RECLAMACION DE BENEFICIOS |
|
POR INCAPACIDAD, COMUNIQUESE CON LA OFICINA MAS CERCANA DE LA |
|
CONTACT THE NEAREST OFFICE OF THE NYS WORKERS' COMPENSATION |
|
JUNTA DE |
COMPENSACION |
OBRERA DE NUEVA YORK, O ESCRIBA A: |
|
BOARD, OR WRITE TO: WORKERS' COMPENSATION BOARD, DISABILITY |
|
WORKERS' |
COMPENSATION |
BOARD, DISABILITY BENEFITS BUREAU,100 |
|
BENEFITS BUREAU, 100 BROADWAY-MENANDS, ALBANY, NY 12241-0005. |
BROADWAY- MENANDS, ALBANY. NY 12241-0005. |
|
|
DB-300 (2-04) Reverse