
Using the online PDF tool by FormsPal, you'll be able to fill in or modify db 802 right here. The tool is continually updated by our team, getting cool functions and growing to be better. Starting is effortless! All you should do is adhere to the following basic steps directly below:
Step 1: Simply click the "Get Form Button" in the top section of this page to open our form editor. This way, you'll find everything that is required to work with your file.
Step 2: Using this advanced PDF editing tool, it is easy to do more than just fill in blanks. Try all of the features and make your documents seem professional with customized textual content added, or optimize the file's original input to perfection - all that supported by the capability to add any kind of graphics and sign the document off.
When it comes to blank fields of this precise document, here is what you should know:
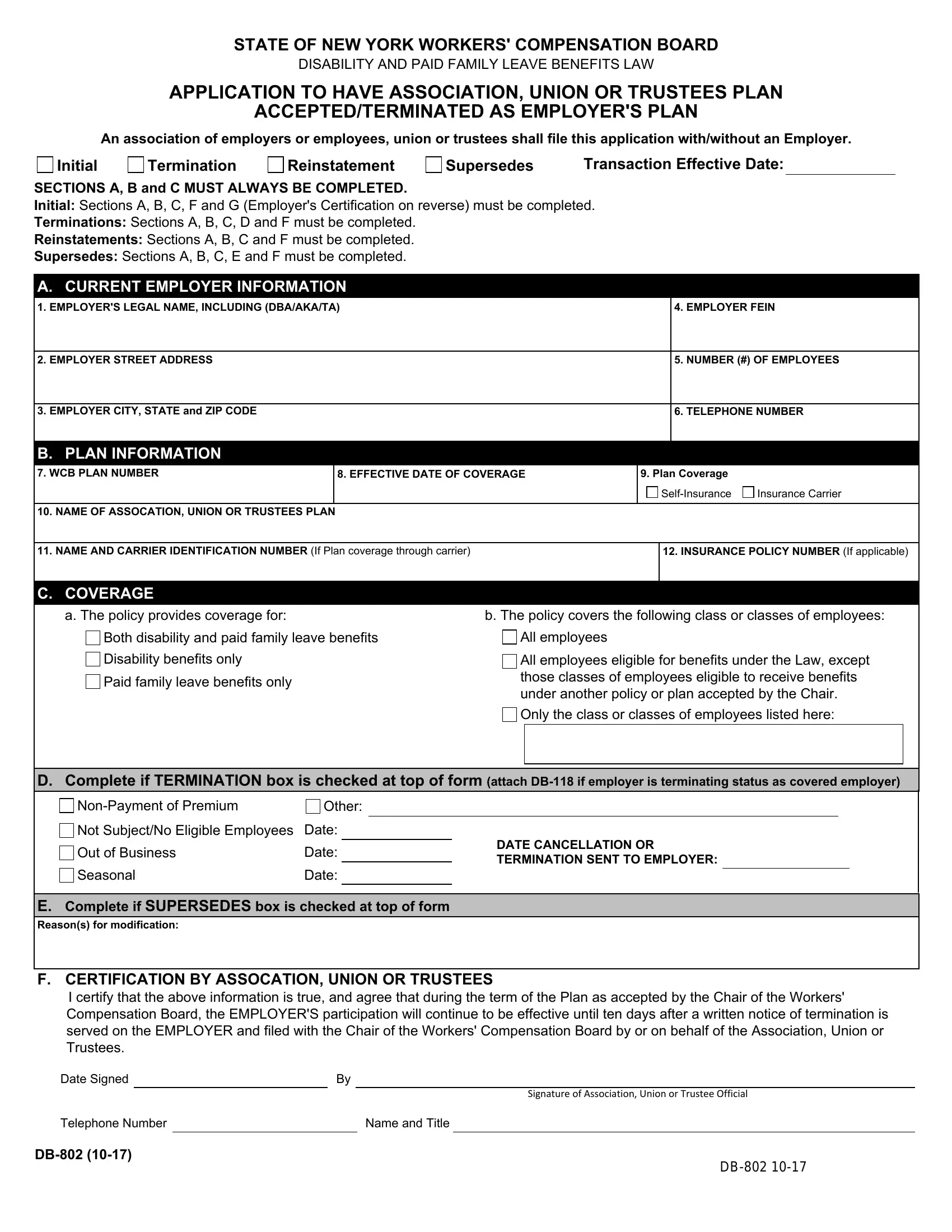
1. Whenever submitting the db 802, make sure to incorporate all essential blanks within its associated section. This will help to expedite the work, enabling your information to be handled quickly and properly.
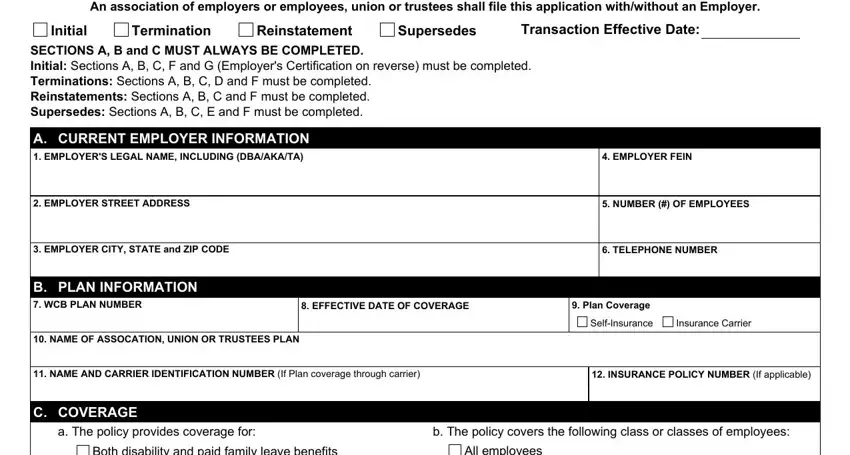
2. Once the previous part is completed, you should add the required specifics in Both disability and paid family, All employees, Disability benefits only, Paid family leave benefits only, All employees eligible for, Only the class or classes of, D Complete if TERMINATION box is, NonPayment of Premium, Other, Not SubjectNo Eligible Employees, Date, Out of Business, Seasonal, Date, and Date so you can move forward further.
In terms of Date and Disability benefits only, make sure that you get them right in this section. Those two are viewed as the key ones in the form.
3. This subsequent part is considered quite easy, - every one of these empty fields needs to be completed here.

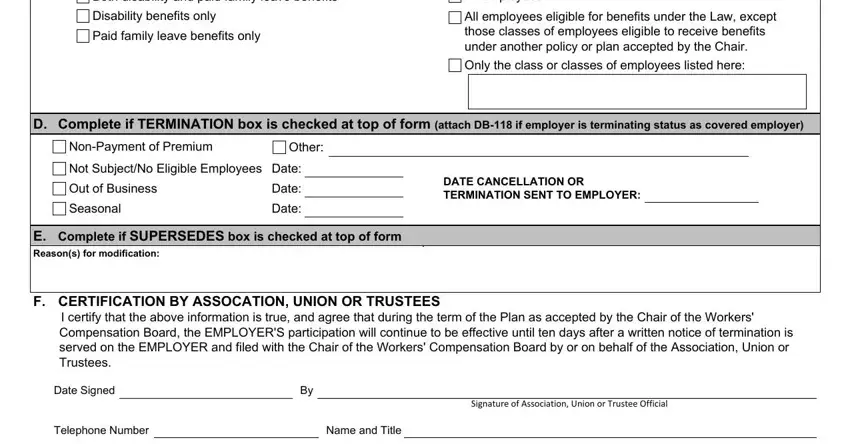
4. This next section requires some additional information. Ensure you complete all the necessary fields - INITIAL CERTIFICATION BY EMPLOYER, State of New York County of, being duly sworn deposes and says, A The EMPLOYER requests acceptance, as the EMPLOYERS Plan, Association Union or Trustees, B The EMPLOYER agrees That all, Disability and Paid Family Leave, That any excess of the aggregate, That unless paid by the, the Workers Compensation Law and, and That the Plan Benefits will be - to proceed further in your process!
5. To wrap up your document, the last section requires a few extra fields. Filling in Date Signed, Employer, Telephone Number, Name and Title, Signature of Owner Partner or, Sworn to before me this, day of, Signature of Notary Public, EMAIL COMPLETED FORM AND, OR MAIL COMPLETED FORM AND, WORKERS COMPENSATION BOARD, PLANS ACCEPTANCE UNIT, PO BOX, and BINGHAMTON NY will certainly conclude everything and you will be done in the blink of an eye!
Step 3: Immediately after double-checking your entries, press "Done" and you're good to go! Get hold of the db 802 after you register online for a 7-day free trial. Easily use the pdf document inside your personal account page, together with any edits and changes being conveniently kept! FormsPal is focused on the privacy of all our users; we make sure all information going through our system is kept protected.