
The DB 450 form can be completed online using FormsPal's free PDF editor. Open the form using the "Get Form" button above, fill in each required field, and download the completed PDF to submit to your employer or NYSIF.
How to fill out the DB 450 form
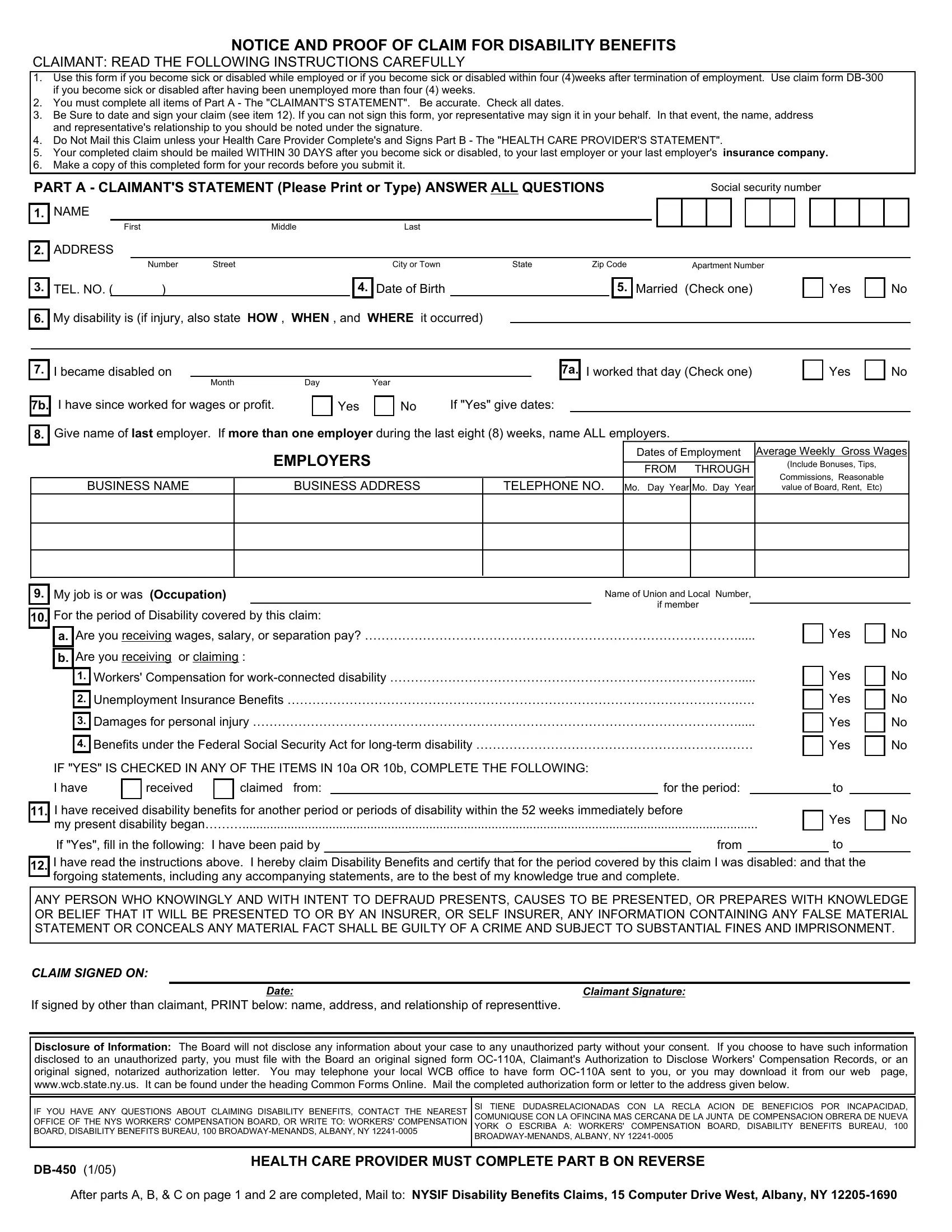
Step 1 - Part A (Claimant Section): Enter your full name, Social Security number, address, and employer details. Provide the date your disability began and describe your illness, injury, or pregnancy. If your condition prevents you from signing, an authorized representative may sign and include a note explaining the situation.
Step 2 - Part B (Health Care Provider Section): Your attending physician or clinic completes this section. They certify your diagnosis, the period of disability, and whether your condition prevents you from working. The doctor must provide their NPI number and sign the form.
Step 3 - Part C (Employer Section): Give the partially completed form to your employer. The employer fills in wage and insurance carrier information, then submits the form to the disability insurer or NYSIF. The employer must complete this section even if they dispute the claim.
Frequently asked questions
Who is eligible to file the DB 450 disability claim?
Employees in New York who are disabled due to a non-work-related illness, injury, or pregnancy while employed, or within four weeks after the last day of paid employment, are eligible to file.
What is the deadline for submitting the form?
Submit the completed form within 30 days from the first day of disability. Filing after 30 days does not automatically disqualify you, but the delay must be explained or your paid benefits may be reduced.
Does the DB 450 form cover New York Paid Family Leave (PFL)?
No. The DB 450 is for short-term disability benefits only. New York PFL requires a separate claim through your employer's PFL insurance carrier. Qualifying employees may receive disability benefits and PFL leave at different times for the same qualifying event.
What if my employer does not carry NYSIF coverage?
Many New York employers use private disability insurance carriers rather than NYSIF. The DB 450 form is used regardless of the carrier. Your employer's HR department or payroll provider can confirm which insurer handles your coverage.