
If you intend to fill out the db300 form, you will not need to install any software - use our online PDF editor instead. We update our tool regularly with user-driven features and welcome your feedback. It only takes a few easy steps:
Step 1: Click the "Get Form" button at the top of this page to open the PDF editor. The form will be ready to complete immediately.
Step 2: Once the PDF editor is open, you can fill in all required fields and also add custom text, modify existing text, insert images, add your signature, and more.
When it comes to the blanks in this specific form, here is what you need to do:
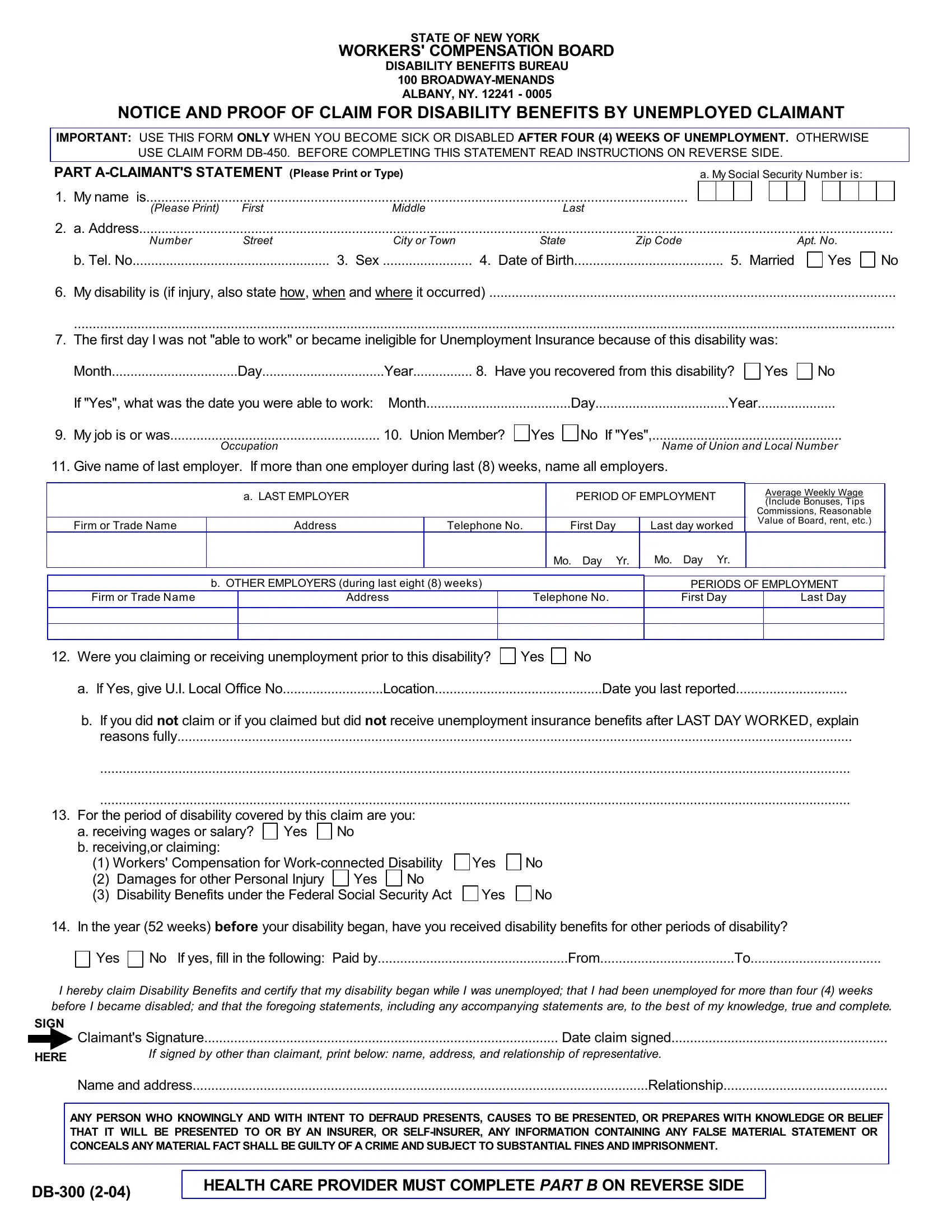
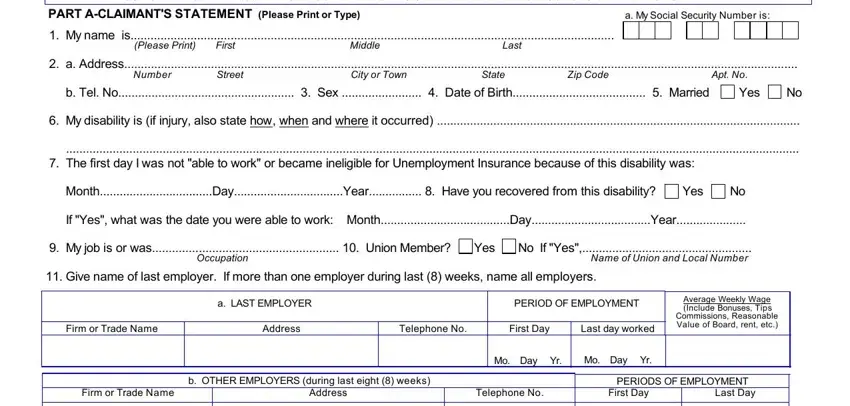
1. It is essential to complete the db300 form properly, so take care when working with these fields:
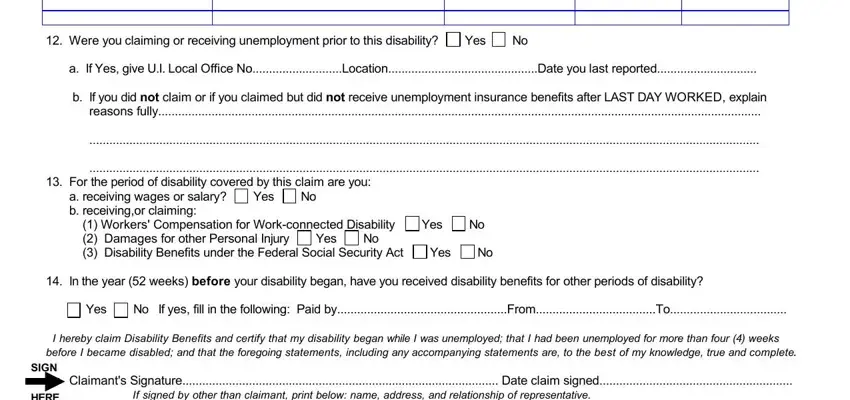
2. Once you complete that section, fill in the following fields: Were you claiming or receiving, a If Yes give UI Local Office, b If you did not claim or if you, For the period of disability, I hereby claim Disability Benefits, SIGN, HERE, and Claimants Signature Date claim. Double-check all entries before continuing.
3. Completing HERE, Claimants Signature Date claim, Name and address Relationship, ANY PERSON WHO KNOWINGLY AND WITH, and HEALTH CARE PROVIDER MUST COMPLETE is essential for the next step. Do not leave any of these blank.

Pay close attention to Claimants Signature Date claim and HERE - these are the key fields in this section.
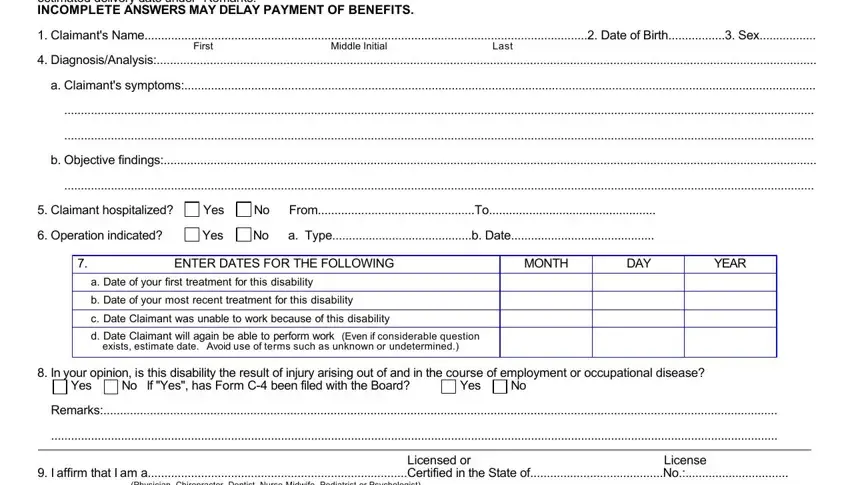
4. This section requires additional information from your health care provider. Make sure to complete: PART B HEALTH CARE PROVIDERS, First Middle Initial Last, DiagnosisAnalysis, a Claimants symptoms, b Objective findings, Claimant hospitalized Yes No, Operation indicated Yes No a, ENTER DATES FOR THE FOLLOWING a, MONTH, DAY, YEAR, In your opinion is this, Remarks, Licensed or License I affirm, and Physician Chiropractor Dentist.
5. The final section is mandatory. Complete all fields including Physician Chiropractor Dentist, Health Care Providers Printed Name, Number Street Citytown State Zip, CLAIMANT READ THESE INSTRUCTIONS, Notification Pursuant to the New, The Workers Compensation Boards, The Board is strongly committed to, personnel and agents in, The Boards Director of Operations, containing personal claimant, Failure to provide the information, social security number enables the, and Disclosure of Information The. An incomplete form may delay processing or result in denial.
Step 3: Review all entries carefully, then click the Done button. You can then download, email, or save the completed form in your FormsPal account. FormsPal protects the privacy of all users and keeps personal data secure.