The Db 450 form serves as a critical notice and proof of claim for individuals seeking disability benefits under specific circumstances, effectively navigating the intersection between employment, health, and legal considerations. Individuals who find themselves sick or disabled while employed, or within four weeks of their employment ending, are directed towards this documentation as a means to articulate their claim for disability benefits. The form is divided into distinct sections, each demanding careful completion by the claimant, their health care provider, and their employer, to ensure the accurate and expedient processing of the claim. Important instructions are provided to guide the claimant through the process, from accurately detailing personal and employment information in Part A, ensuring the health care provider completes Part B, to submitting the claim within thirty days from the onset of disability. The emphasis on timely, precise submission, along with instructions for individuals unable to sign the form themselves, underscores the system's effort to accommodate diverse needs while safeguarding against fraudulent claims. Additionally, the form encapsulates a broader framework that manages the interplay between disability and employment - reflecting on workers' rights, employer responsibilities, and the healthcare system's role in certifying the conditions that warrant such benefits. It portrays a structured approach towards ensuring that individuals navigating health challenges in the context of employment receive due consideration and support as envisaged by law.
| Question | Answer |
|---|---|
| Form Name | Db 450 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | DB 450 Claim Form db hr form |
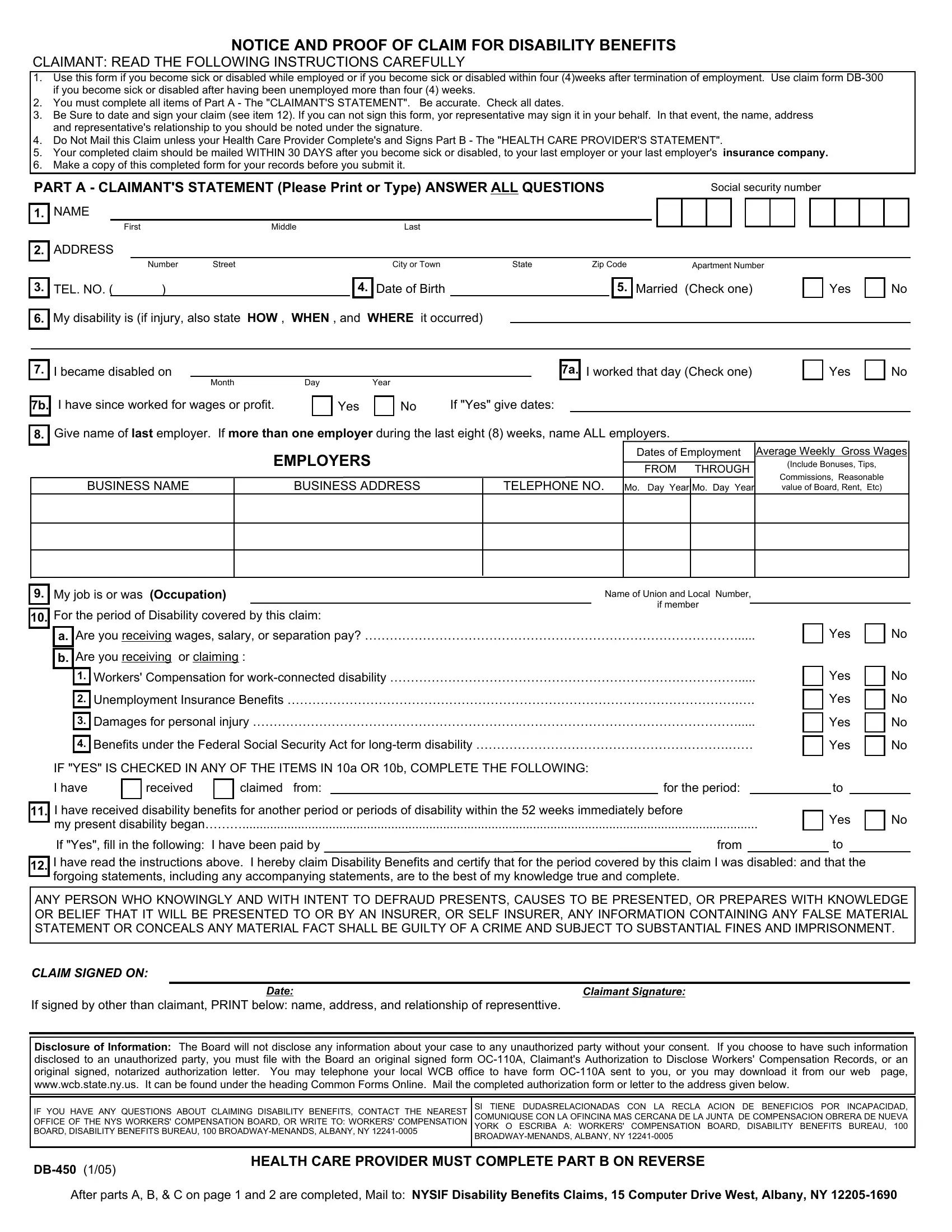
NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS
CLAIMANT: READ THE FOLLOWING INSTRUCTIONS CAREFULLY
1.Use this form if you become sick or disabled while employed or if you become sick or disabled within four (4)weeks after termination of employment. Use claim form
2.You must complete all items of Part A - The "CLAIMANT'S STATEMENT". Be accurate. Check all dates.
3.Be Sure to date and sign your claim (see item 12). If you can not sign this form, yor representative may sign it in your behalf. In that event, the name, address and representative's relationship to you should be noted under the signature.
4.Do Not Mail this Claim unless your Health Care Provider Complete's and Signs Part B - The "HEALTH CARE PROVIDER'S STATEMENT".
5.Your completed claim should be mailed WITHIN 30 DAYS after you become sick or disabled, to your last employer or your last employer's insurance company.
6.Make a copy of this completed form for your records before you submit it.
PART A - CLAIMANT'S STATEMENT (Please Print or Type) ANSWER ALL QUESTIONS |
|
|
|
Social security number |
||||||||
1. NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
First |
Middle |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
2.ADDRESS
|
|
|
Number |
Street |
|
City or Town |
State |
Zip Code |
Apartment Number |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
TEL. NO. ( |
) |
|
|
4. |
Date of Birth |
|
|
|
5. |
Married (Check one) |
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No
6.
My disability is (if injury, also state HOW , WHEN , and WHERE it occurred)
7.
7b.
8.
I became disabled on |
|
|
|
|
|
|
|
|
7a. |
I worked that day (Check one) |
|
Yes |
|
Month |
Day |
Year |
|
|
|
|
|
|
|||
|
If "Yes" give dates: |
|
|
|||||||||
I have since worked for wages or profit. |
|
|
Yes |
|
No |
|
|
|||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Give name of last employer. If more than one employer during the last eight (8) weeks, name ALL employers.
No
BUSINESS NAME
EMPLOYERS
BUSINESS ADDRESS
TELEPHONE NO.
Dates of Employment
FROM THROUGH
Mo. Day Year Mo. Day Year
Average Weekly Gross Wages
(Include Bonuses, Tips,
Commissions, Reasonable value of Board, Rent, Etc)
9.
10.
My job is or was (Occupation) |
|
Name of Union and Local Number, |
For the period of Disability covered by this claim: |
if member |
|
|
||
a.Are you receiving wages, salary, or separation pay? ……………………………………………………………………………….....
b.Are you receiving or claiming :
1.Workers' Compensation for
2.Unemployment Insurance Benefits ……………………………………………………………………………………………….….
3.Damages for personal injury ……………………………………………………………………………………………………….....
4.Benefits under the Federal Social Security Act for
IF "YES" IS CHECKED IN ANY OF THE ITEMS IN 10a OR 10b, COMPLETE THE FOLLOWING:
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
I have |
|
received |
|
claimed from: |
|
for the period: |
|
|
|
|
|
|
|
11.I have received disability benefits for another period or periods of disability within the 52 weeks immediately before
my present disability began……….....................................................................................................................................................
If "Yes", fill in the following: I have been paid by |
from |
to
Yes
to
No
12.
I have read the instructions above. I hereby claim Disability Benefits and certify that for the period covered by this claim I was disabled: and that the forgoing statements, including any accompanying statements, are to the best of my knowledge true and complete.
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD PRESENTS, CAUSES TO BE PRESENTED, OR PREPARES WITH KNOWLEDGE OR BELIEF THAT IT WILL BE PRESENTED TO OR BY AN INSURER, OR SELF INSURER, ANY INFORMATION CONTAINING ANY FALSE MATERIAL STATEMENT OR CONCEALS ANY MATERIAL FACT SHALL BE GUILTY OF A CRIME AND SUBJECT TO SUBSTANTIAL FINES AND IMPRISONMENT.
CLAIM SIGNED ON:
Date: |
Claimant Signature: |
If signed by other than claimant, PRINT below: name, address, and relationship of representtive.
Disclosure of Information: The Board will not disclose any information about your case to any unauthorized party without your consent. If you choose to have such information disclosed to an unauthorized party, you must file with the Board an original signed form
IF YOU HAVE ANY QUESTIONS ABOUT CLAIMING DISABILITY BENEFITS, CONTACT THE NEAREST OFFICE OF THE NYS WORKERS' COMPENSATION BOARD, OR WRITE TO: WORKERS' COMPENSATION BOARD, DISABILITY BENEFITS BUREAU, 100
SI TIENE DUDASRELACIONADAS CON LA RECLA ACION DE BENEFICIOS POR INCAPACIDAD, COMUNIQUSE CON LA OFINCINA MAS CERCANA DE LA JUNTA DE COMPENSACION OBRERA DE NUEVA YORK O ESCRIBA A: WORKERS' COMPENSATION BOARD, DISABILITY BENEFITS BUREAU, 100
HEALTH CARE PROVIDER MUST COMPLETE PART B ON REVERSE
After parts A, B, & C on page 1 and 2 are completed, Mail to: NYSIF Disability Benefits Claims, 15 Computer Drive West, Albany, NY
NOTICE OF PROOF OF CLAIM FOR DISABILITY BENEFITS - IMPORTANT: Use this form only when the claimant becomes sick or disable while employed or becomes sick or disabled within four(4) weeks after termination of employment. Otherwise use the green claim form
Part B - Health Care Provider's Statement (Please Print or Type)- The Health Care Provider's Statement must be filled in completely and the
Form mailed to the Insurance Carrier or
1.
4.
5.
6.
7.
Claimant's Name: |
|
|
|
|
2. |
Age |
|
|
|
3. |
Sex |
|
|
|
|
||
|
First |
Middle |
Last |
|
|
|
|
|
|
|
Male |
Female |
|||||
Diagnosis / Analysis: |
|
|
|
|
|
|
|
Diagnosis Code: |
|
|
|
|
|||||
a.Claimant's Symptom's:
b.Objective Findings:
c.If Disability is pregnancy related, enter ESTIMATED DELIVERY DATE .
Claimant Hospitalized? |
|
Yes |
|
No |
Date from: |
|
|
|
to |
|
|
|
||||||
Operation indicated? |
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
a. Type |
|
|
|
|
|
b. Date |
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter Dates for the following: |
|
|
|
|
|
|
|
|
|
Month |
|
|
|
Day |
Year |
|||
a.Date of your first treatment for this Disability …………........................................………
b.Date of your most recent treatment for this Disability ……….....................................…
c.Date claimant was unable to work because of this Disability …...............................…
d. Date claimant will be able to perform usual work**………….................................…..
**Even if considerable question exists, ESTIMATE DATE . Avoid the use of terms such as unknown or undetermined.
**
8.In your opinion is this Disability the result of injury arising out of the course of employment or occupational disease?
a.If yes, has Form
Remarks:
Yes
Yes
No
No
I affirm that |
Chiropractor |
Physician |
Psychologist |
Licensed in the State of: |
License Number: |
I am a: |
Dentist |
Podiatrist |
|
|
|
|
|
|
|
|
|
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD PRESENTS, CAUSES TO BE PRESENTED, OR PREPARES WITH KNOWLEDGE OR BELIEF THAT IT WILL BE PRESENTED TO OR BY AN INSURER, OR SELF INSURER ANY INFORMATION CONTAINING ANY FALSE MATERIAL STATEMENT OR CONCEALS ANY MATERIAL FACT SHALL BE QUILTY OF A CRIME AND SUBJECT TO SUBSTANCIAL FINES AND IMPRISONMENT.
Health Care Provider 's Signature |
|
|
|
|
|
Date: |
|||
Health Care Provider's Name (Please Print) |
|
|
|
|
Phone No. |
||||
Office Address: |
|
|
|
|
|
|
|
||
|
Number Street |
Apt/Suite |
City/Town |
State |
Zip Code |
||||
HIPPA NOTICE - In order to adjudicate a workers' compensation claim, WCL
Part C - EMPLOYER'S STATEMENT
1. |
Employee's Name: |
2. |
Soc.Sec. No: |
||
|
|
|
|
|
|
3.Employee's Address:
|
|
|
|
|
|
Number |
|
|
Street |
|
|
|
|
|
|
|
|
|
|
Apartment Number |
|
|
|
|
|
|
|
|
|
City / Town |
|
|
|
|
|
State |
|
|
|
Zip Code |
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Employee's Occupation: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Date of Hire: |
|
|
|
|
|
|
|
|
|
6. |
Status: |
|
|
|
Full Time |
|
|
|
Part Time |
|
|
||||||||||||||||||||
7. |
Is the Claimant an: |
|
|
Owner |
|
|
Officer |
|
Partner |
|
|
|
Employee |
|
|
|
High School Student |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Indicate the employee's normal work schedule: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
8. |
|
|
|
Mon |
|
|
|
Tues |
|
|
|
Wed |
|
|
|
Thur |
|
|
|
|
Fri |
|
|
|
Sat |
|
|
|
Sun |
|
|
|
|
|||||||||||||||||||||||||
9. |
If the employee is no longer in your employ, explain why: |
|
|
|
Quit? |
|
|
|
Discharged? |
|
|
Labor Dispute? |
|
|
|
|
Lack of Work? |
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
If Quit or Discharged explain why |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you expect to rehire him/her? |
|
|
Yes |
|
No |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. |
Date Employee last worked: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weekly Wages 8 Weeks prior to Disability |
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(include value of Board, Lodging, and Tips if any) |
|
|
|||||||||||||||||
11. |
Date Employee's Wages Ceased: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
12. |
Date Employee Returned to Work: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Week Ending |
|
|
No. of Days |
|
GROSS WEEKLY WAGES |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Month |
Day |
|
|
Year |
Worked |
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
13. |
Are Wages being Continued during Disability? ………… |
|
|
|
Yes |
|
No |
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
14. |
If YES , are you requesting reimbursement?.....…………… |
|
|
|
Yes |
|
No |
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
15. |
Is Employee receiving or claiming Unemployment Ins? …… |
|
|
|
Yes |
|
No |
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
16. |
Is Employee receiving or claiming Workers' Comp. Ins? … |
|
|
|
Yes |
|
No |
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
17. |
Did this Disability occur as a result of employment? ………… |
|
|
|
Yes |
|
No |
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
18. |
Is Employee in a Union providing Disability Benefits? ……… |
|
|
|
Yes |
|
No |
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
19. |
Are you aware of other employment claimant may have? |
|
|
|
Yes |
|
No |
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
20. |
Did Employee receive |
PAID SICK TIME during disability? |
|
|
|
Yes |
|
|
No |
8. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
If YES, provide dates of paid sick time: From: |
|
|
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION: |
|
|
|
|
NYSIF DISABILITY POLICY NUMBER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Employer NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax No. |
|
|
|
|
|
|
|
|
|||||||||||
ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
SIGNATURE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title: |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||