
You'll be able to fill in form dd2168 effortlessly by using our online PDF tool. To make our tool better and simpler to use, we consistently develop new features, taking into account suggestions from our users. To begin your journey, consider these easy steps:
Step 1: Press the "Get Form" button above on this webpage to open our tool.
Step 2: With this online PDF tool, it is easy to do more than merely complete blank form fields. Edit away and make your docs seem faultless with custom text put in, or tweak the file's original content to excellence - all that comes with an ability to add any kind of graphics and sign the file off.
Filling out this PDF needs attention to detail. Ensure all necessary fields are done correctly.
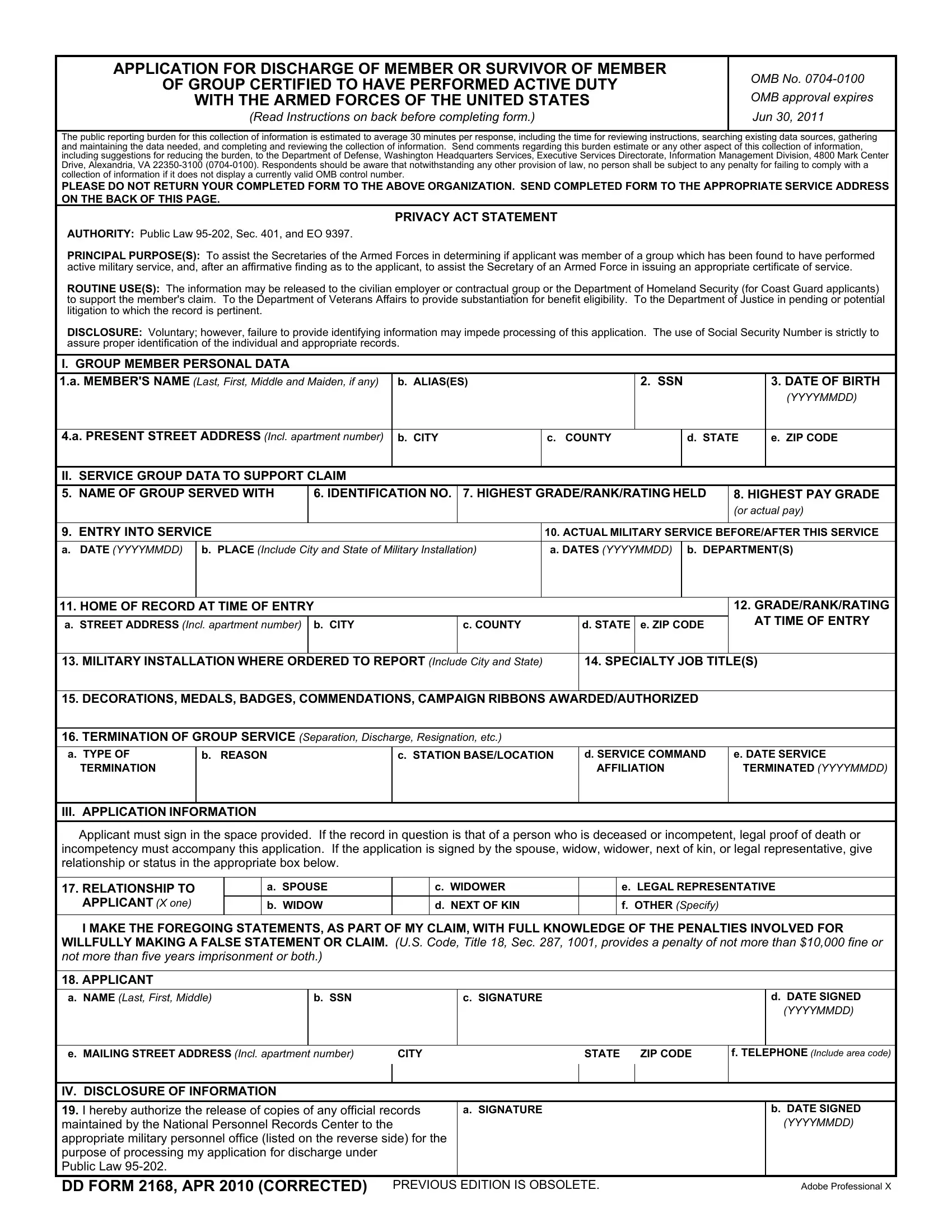
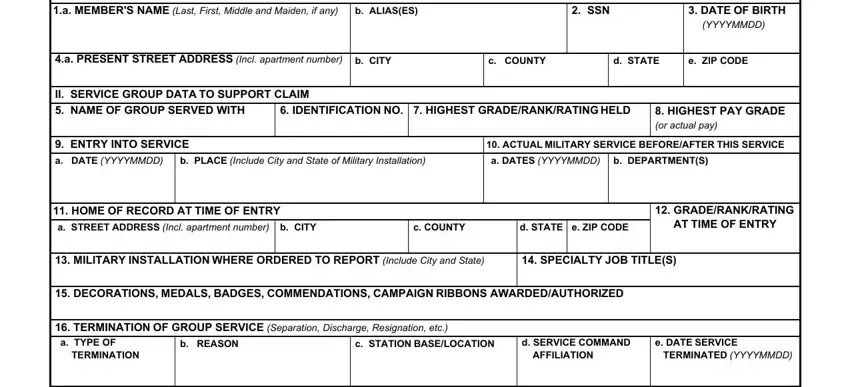
1. The form dd2168 involves certain information to be entered. Make sure the next blanks are filled out:
2. Immediately after the last part is completed, go to type in the applicable details in these - III APPLICATION INFORMATION, a SPOUSE b WIDOW, RELATIONSHIP TO APPLICANT X one I, e LEGAL REPRESENTATIVE f OTHER, c WIDOWER d NEXT OF KIN, c SIGNATURE, b SSN, d DATE SIGNED YYYYMMDD, e MAILING STREET ADDRESS Incl, CITY, STATE, ZIP CODE, f TELEPHONE Include area code, IV DISCLOSURE OF INFORMATION I, and a SIGNATURE.
People who use this document often make errors while completing c SIGNATURE in this section. Remember to read twice what you type in here.
Step 3: Before moving forward, make certain that form fields have been filled out the correct way. Once you think it's all good, click “Done." Join FormsPal today and immediately access form dd2168, all set for download. All adjustments you make are kept , making it possible to change the form at a later point if necessary. FormsPal ensures your information privacy via a protected system that never saves or shares any kind of personal information involved in the process. Feel safe knowing your documents are kept confidential whenever you work with our tools!