

Using PDF documents online is definitely a breeze using our PDF tool. You can fill out 1999 here in a matter of minutes. Our tool is constantly developing to grant the best user experience attainable, and that is due to our commitment to continuous improvement and listening closely to feedback from users. To get the process started, take these simple steps:
Step 1: Just click on the "Get Form Button" above on this page to launch our pdf editing tool. There you'll find all that is needed to work with your file.
Step 2: With our handy PDF editing tool, you are able to accomplish more than merely fill in blank form fields. Edit away and make your forms look high-quality with custom textual content incorporated, or tweak the file's original content to perfection - all that comes along with an ability to insert your personal graphics and sign the file off.
It's straightforward to finish the form adhering to our helpful tutorial! This is what you have to do:
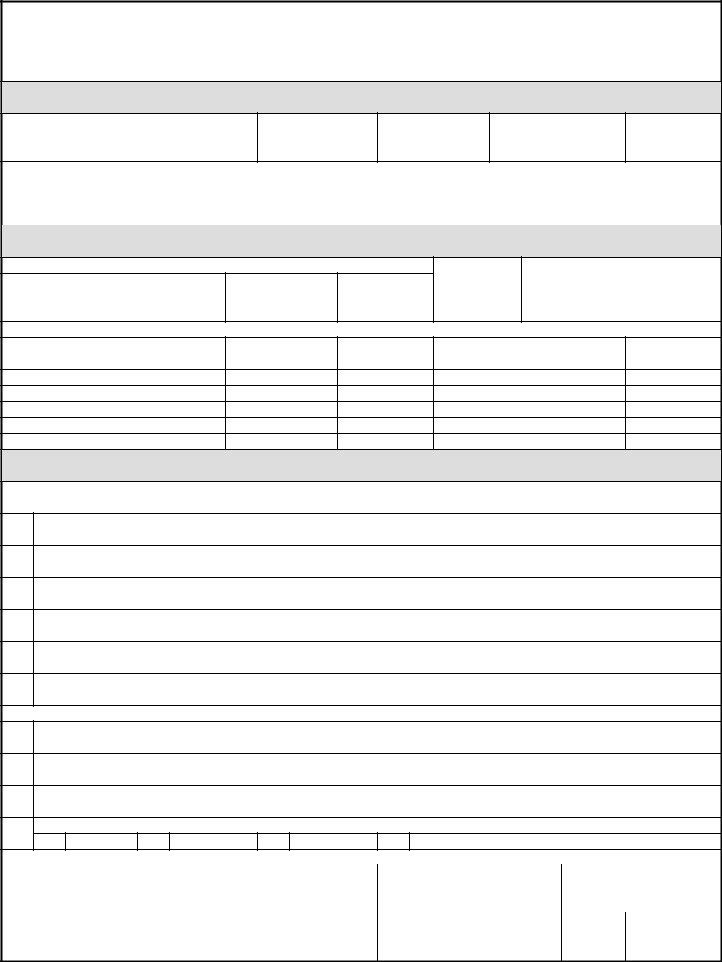
1. Complete your 1999 with a group of major fields. Collect all the important information and be sure not a single thing overlooked!
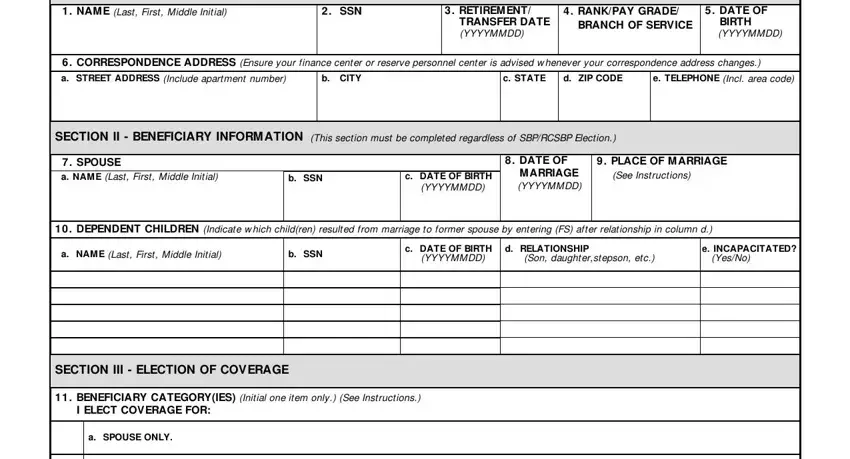
2. After finishing the previous part, go on to the next step and enter the essential particulars in all these fields - b SPOUSE AND CHILDREN, c CHILDREN ONLY, d NATURAL PERSON WITH INSURABLE, e FORM ER SPOUSE Complete DD, Coast Guard, f FORM ER SPOUSE AND DEPENDENT, Former Spouse Coverage or the, LEVEL OF COVERAGE Initial one, a I ELECT COVERAGE BASED ON FULL, b I ELECT COVERAGE BASED ON A, See Instructions, c I ELECT TO INCREASE M Y CURRENT, Enter desired base amount, d I ELECT COVERAGE BASED ON FULL, and INSURABLE INTEREST BENEFICIARY.
Many people often make errors while filling in d NATURAL PERSON WITH INSURABLE in this part. You should read again what you enter right here.
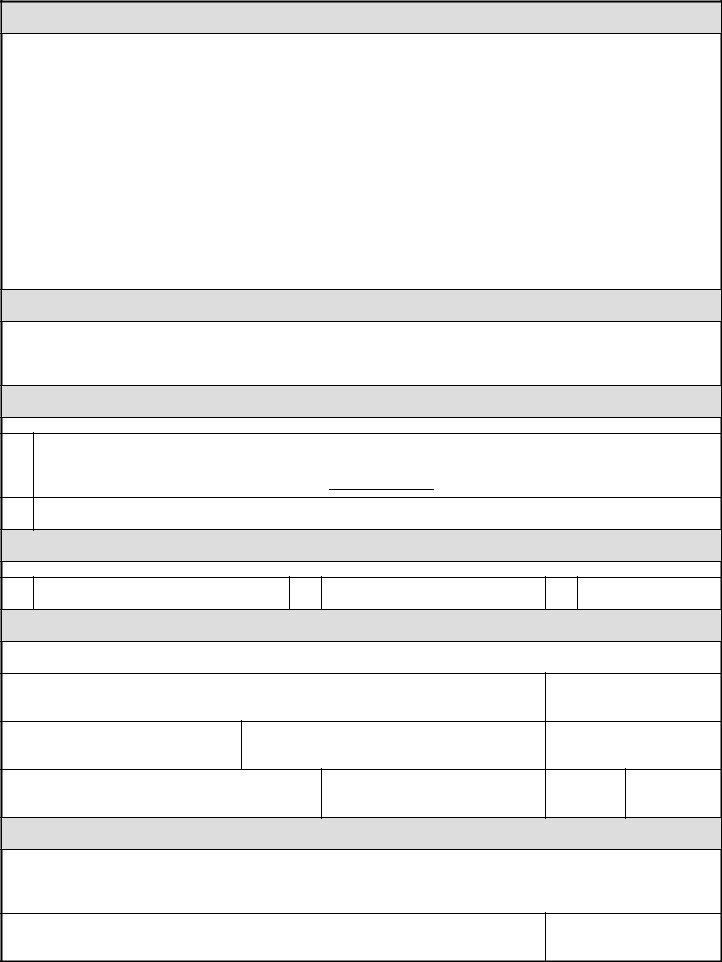
3. This next step is focused on e STREET ADDRESS Include apartment, f CITY, g STATE, h ZIP CODE, DD FORM M AR EG, and WHSDIOR Mar - fill in every one of these fields.

4. All set to fill out this fourth part! Here you've got all these USE THIS SECTION TO CONTINUE AN, SECTION V M ARITAL STATUS HISTORY, INDICATE DATES OF PREVIOUS M, and SECTION VI ENROLLM ENT PREM IUM blank fields to do.
5. This final section to finish this PDF form is pivotal. Make certain you fill out the mandatory blanks, including ENROLLM ENT PREM IUM OPTIONS, a IM M EDIATE FULL ENROLLM ENT, payment attached, b IM M EDIATE PARTIAL ENROLLM ENT, payment attached The remainder due, c FULL ENROLLM ENT PREM IUM AM, SECTION VII M EM BER OF A RESERVE, I ELECT RESERVE COM PONENT, a CHANGE M Y ELECTION FROM, b DEFERRED ANNUITY UNTIL AGE, IM M EDIATE ANNUITY from Option B, Option B, c IM M EDIATE ANNUITY, Option C, and SECTION VIII SPOUSE CONCURRENCE, before finalizing. Failing to do so might contribute to an incomplete and probably unacceptable paper!
Step 3: Just after taking one more look at your fields and details, hit "Done" and you're good to go! Join us right now and instantly get access to 1999, set for download. All adjustments you make are saved , allowing you to customize the document further if necessary. When using FormsPal, you'll be able to complete documents without stressing about personal data incidents or data entries being distributed. Our secure system helps to ensure that your private information is maintained safely.