
When working in the online tool for PDF editing by FormsPal, it is possible to fill in or alter de 542 form right here. To maintain our editor on the leading edge of efficiency, we strive to put into practice user-oriented capabilities and improvements on a regular basis. We're at all times looking for feedback - assist us with revampimg PDF editing. It just takes just a few simple steps:
Step 1: Simply hit the "Get Form Button" in the top section of this webpage to launch our pdf form editor. There you'll find everything that is needed to work with your file.
Step 2: As you launch the tool, you will notice the form all set to be filled out. Aside from filling out different blank fields, you might also do various other actions with the Document, specifically adding any words, changing the initial text, inserting illustrations or photos, affixing your signature to the form, and a lot more.
This PDF doc needs some specific information; in order to guarantee consistency, please be sure to pay attention to the suggestions listed below:
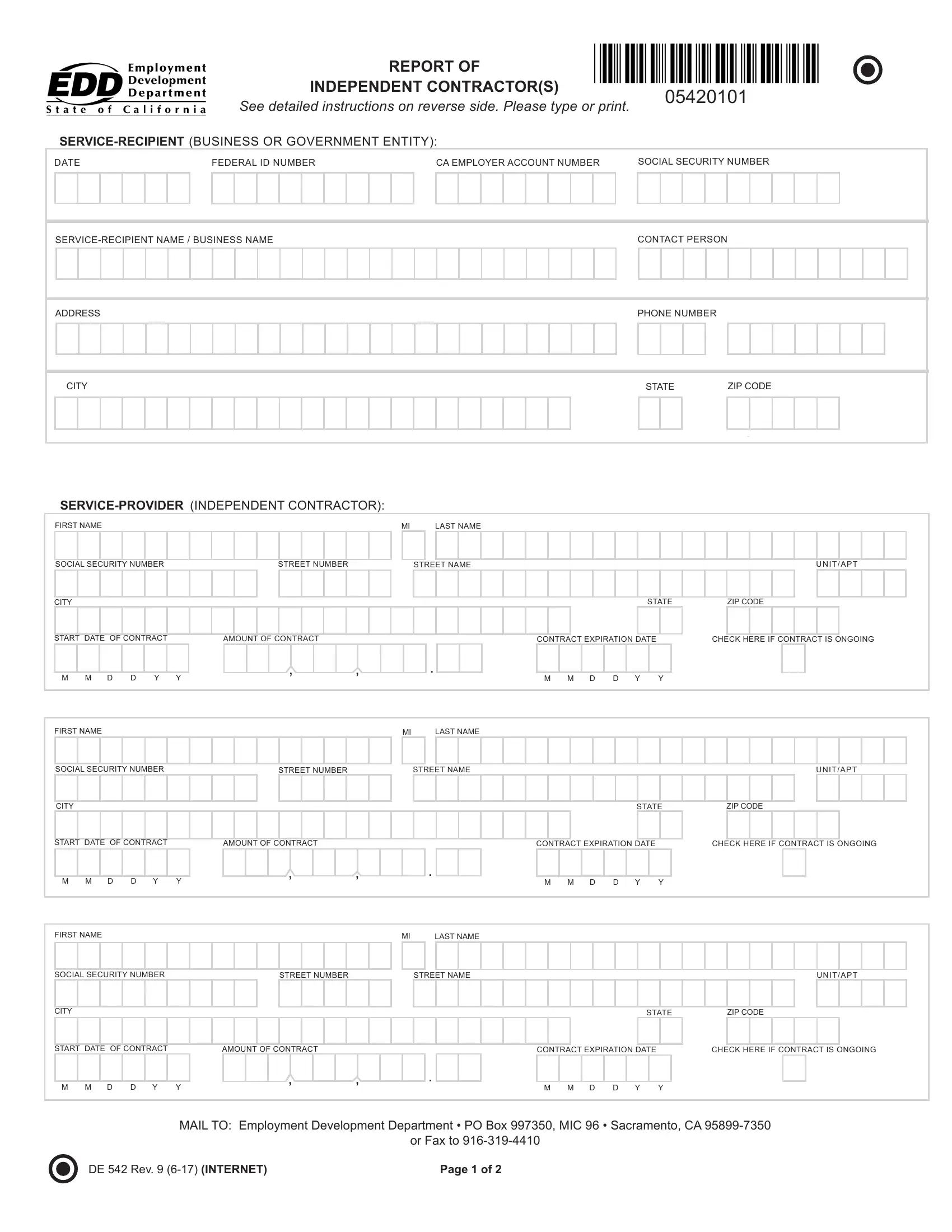
1. While submitting the de 542 form, be certain to complete all important blanks within its corresponding section. It will help speed up the process, allowing for your details to be handled without delay and accurately.
2. Once your current task is complete, take the next step – fill out all of these fields - START DATE OF CONTRACT, AMOUNT OF CONTRACT, CONTRACT EXPIRATION DATE, CHECK HERE IF CONTRACT IS ONGOING, FIRST NAME, LAST NAME, SOCIAL SECURITY NUMBER, STREET NUMBER, STREET NAME, U N I T A P T, CITY, STATE, ZIP CODE, START DATE OF CONTRACT, and AMOUNT OF CONTRACT with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Be extremely careful while filling in CONTRACT EXPIRATION DATE and LAST NAME, as this is where a lot of people make a few mistakes.
Step 3: After you have looked again at the details in the file's blanks, just click "Done" to finalize your form at FormsPal. Grab your de 542 form the instant you register at FormsPal for a free trial. Conveniently view the pdf form within your personal account page, along with any modifications and adjustments conveniently preserved! At FormsPal.com, we do our utmost to guarantee that all your details are maintained protected.