
Working with the DFA 1239 is straightforward using our online PDF editor. FormsPal provides a complete experience for managing California Department of Social Services forms. Our team of document specialists has reviewed this form to provide accurate guidance for every step. No downloads or software installation is required.
Step 1: Open the PDF Editor
Click the "Get Form" button at the top of this page to access our PDF editor. The tool opens directly in your browser. You do not need to create an account or provide personal information to get started. The editor is designed for speed and ease of use on any device.
Step 2: Fill Out the Required Fields
Our advanced PDF editor allows you to complete all blank fields and modify existing information. You can add custom text, adjust entries, insert graphics, and sign the document electronically. Take your time and be careful when filling out each section.
Pay close attention when completing the following fields in this section:
Fill in all of the following fields carefully: Approval, DenialWithdrawal, As of your CalFresh benefits are, As of the CalFresh, each month, MMDDCCYY, Because your CalWORKs case has, MMCCYY, MMCCYY, This replaces your previous, Your Transitional CalFresh, Reporting, You are encouraged to report if, Recertification, and You will get a notice when it is.
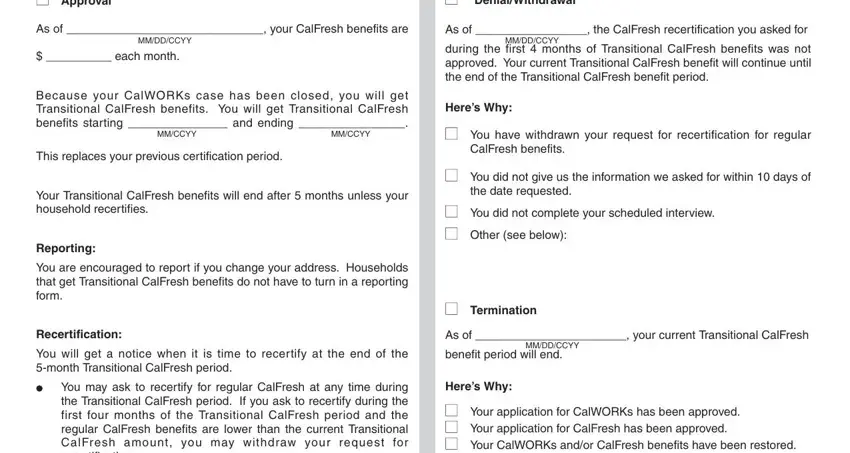
It is easy to make an error in the Recertification section. Double-check all entries before moving to the next section.
Step 3: Complete the Required Form Sections
This part requires you to fill in all fields in You may review them at your, CF REQUIRED FORM SUBSTITUTE, and Page of. Make sure each entry is accurate and complete before continuing.

Step 4: Enter Hearing Request Information
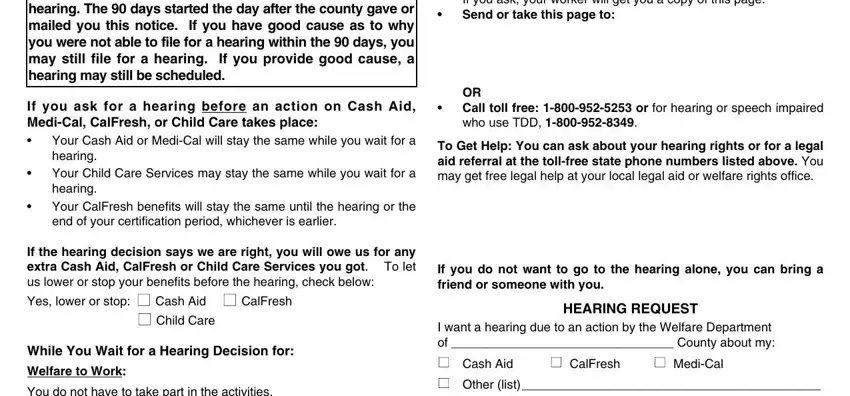
If you need to request a state hearing to contest a department decision, complete the following required fields: cid, cid, If you ask your worker will get, OR Call toll free or for hearing, To Get Help You can ask about your, If you do not want to go to the, HEARING REQUEST, I want a hearing due to an action, CalFresh, MediCal, You have the right to ask for a, If you ask for a hearing before an, Your Cash Aid or MediCal will stay, cid, cid, and If the hearing decision says we.
Step 5: Finalize and Submit Your Form
The final section is critical. Make sure all required fields are complete before submitting. Fill in the following: Heres Why, n If you need more space check, n I need the state to provide me, A relative or friend cannot, My language or dialect is, NAME OF PERSON WHOSE BENEFITS WERE, BIRTH DATE, STREET ADDRESS, PHONE NUMBER, STATE, ZIP CODE, DATE, You may receive child care, If we told you your other, and If we told you we will pay your.
Click "Done" when all fields are complete. Your form is saved automatically. You can return to edit the document at any time. FormsPal does not share any personal information or data you enter with third parties.
Common Questions About CalFresh Benefits Forms
What does the DFA 1239 notice tell me?
This notice tells you whether your Transitional CalFresh benefits have been approved, denied, or terminated. It also explains the reasons for the decision and the steps you can take if you disagree. The notice includes the duration of your benefits and any recertification requirements.
What should I do if I receive a denial notice?
If your benefits are denied, you have the right to request a state hearing. Complete the Hearing Request section of this form and submit it before the deadline shown on the notice. You can also call the toll-free number listed on the document to speak with a caseworker or social services representative.
How long do Transitional CalFresh benefits last?
The duration of your Transitional CalFresh benefits depends on your household's specific situation and eligibility at the time of your CalWORKs case closure. The notice will include the exact benefit period and any recertification dates. You will receive a notice from the department when it is time to renew or recertify your benefits.
Do I need to verify my information after submission?
Yes. The department may request verification of your household income, size, or other eligibility information at any time during your benefit period. Keep copies of all documents you submit and respond promptly to any department requests. Delays in providing verification can interrupt your food assistance benefits.
What other CalFresh forms might I need?
Depending on your situation, you may also need to complete other related forms. The CalFresh application form is required for new applicants. The CalFresh renewal form is used to extend existing benefits. You may also need the DFA SNAP 2 form for supplemental nutrition assistance program requirements.
Related California Social Services Forms
FormsPal provides access to a wide range of California social services forms. Here are some additional resources that may be helpful for managing your benefits and assistance programs:
- CalFresh Application Form - Apply for CalFresh food assistance benefits in California
- CalFresh Renewal Form - Renew your existing CalFresh benefits before they expire
- DFA SNAP 2 Form - Complete your Supplemental Nutrition Assistance Program application
- DFA Form 756 - Additional California Department of Social Services assistance form