
When working in the online PDF editor by FormsPal, you're able to complete or modify michigan 54a right here. In order to make our editor better and less complicated to utilize, we continuously design new features, with our users' suggestions in mind. With some basic steps, you may begin your PDF editing:
Step 1: Access the PDF file inside our tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: This tool will allow you to work with your PDF in a variety of ways. Transform it with any text, correct original content, and include a signature - all doable within a few minutes!
This PDF doc will require specific details; in order to guarantee correctness, be sure to take into account the next guidelines:
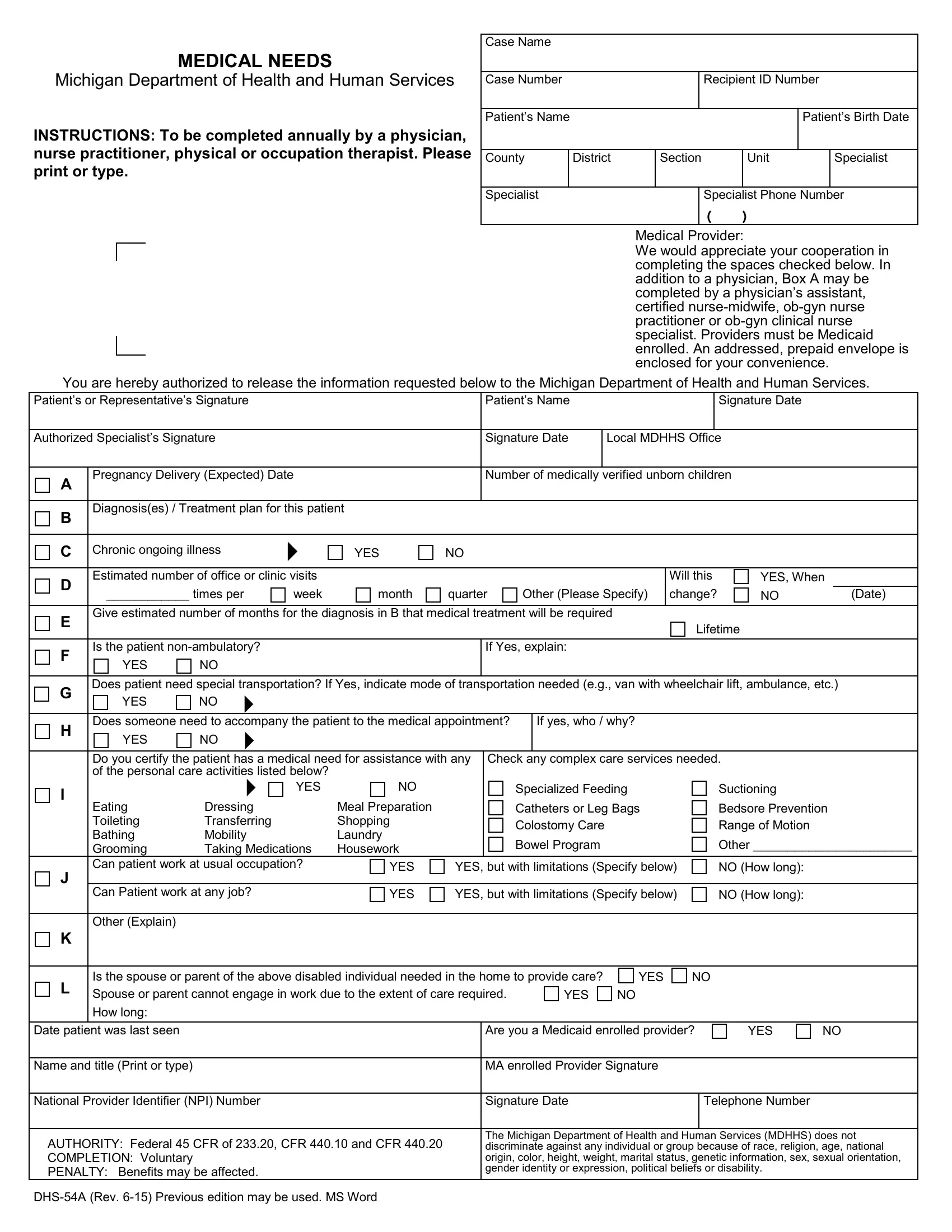
1. The michigan 54a requires specific information to be entered. Be sure that the following blank fields are finalized:
2. After completing the previous section, head on to the next step and fill out all required details in these blanks - Authorized Specialists Signature, Pregnancy Delivery Expected Date, Diagnosises Treatment plan for, C Chronic ongoing illness YES, Signature Date, Local MDHHS Office, Number of medically verified, Estimated number of office or, Will this, times per, week, month, quarter, Other Please Specify, and change.
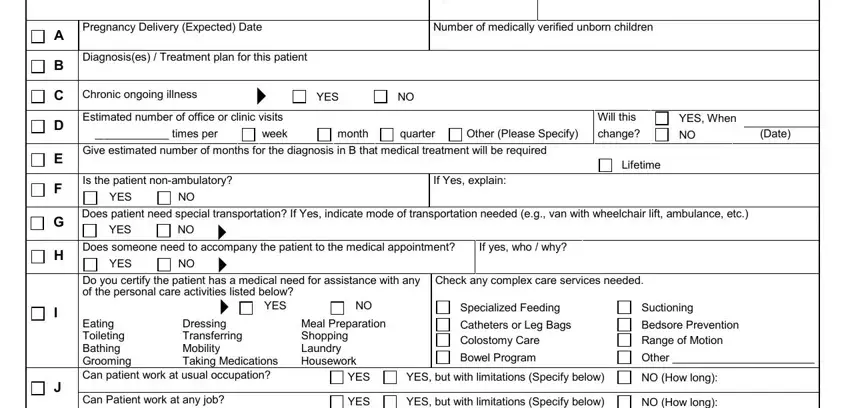
3. Throughout this stage, examine Eating Toileting Bathing Grooming, Is the spouse or parent of the, YES, YES, Date patient was last seen, Name and title Print or type, National Provider Identifier NPI, AUTHORITY Federal CFR of CFR, DHSA Rev Previous edition may be, Are you a Medicaid enrolled, YES, MA enrolled Provider Signature, Signature Date, Telephone Number, and The Michigan Department of Health. All these will need to be filled out with utmost accuracy.
People generally make some mistakes while completing Eating Toileting Bathing Grooming in this part. You need to re-examine everything you enter right here.
Step 3: Spell-check what you've entered into the form fields and click the "Done" button. After starting a7-day free trial account with us, you will be able to download michigan 54a or send it via email directly. The PDF form will also be available through your personal account with your each edit. We don't sell or share any details that you provide whenever working with documents at our website.