
Using PDF forms online is always super easy using our PDF tool. Anyone can fill out pennsylvania 124 form here with no trouble. To retain our tool on the forefront of practicality, we work to put into action user-driven capabilities and improvements regularly. We're at all times looking for suggestions - join us in revolutionizing PDF editing. This is what you would have to do to begin:
Step 1: Firstly, access the tool by pressing the "Get Form Button" at the top of this page.
Step 2: With this handy PDF file editor, you're able to accomplish more than simply fill out blanks. Express yourself and make your forms seem perfect with customized textual content added in, or modify the original input to perfection - all comes along with the capability to incorporate your own graphics and sign it off.
It is an easy task to complete the pdf using this practical tutorial! This is what you must do:
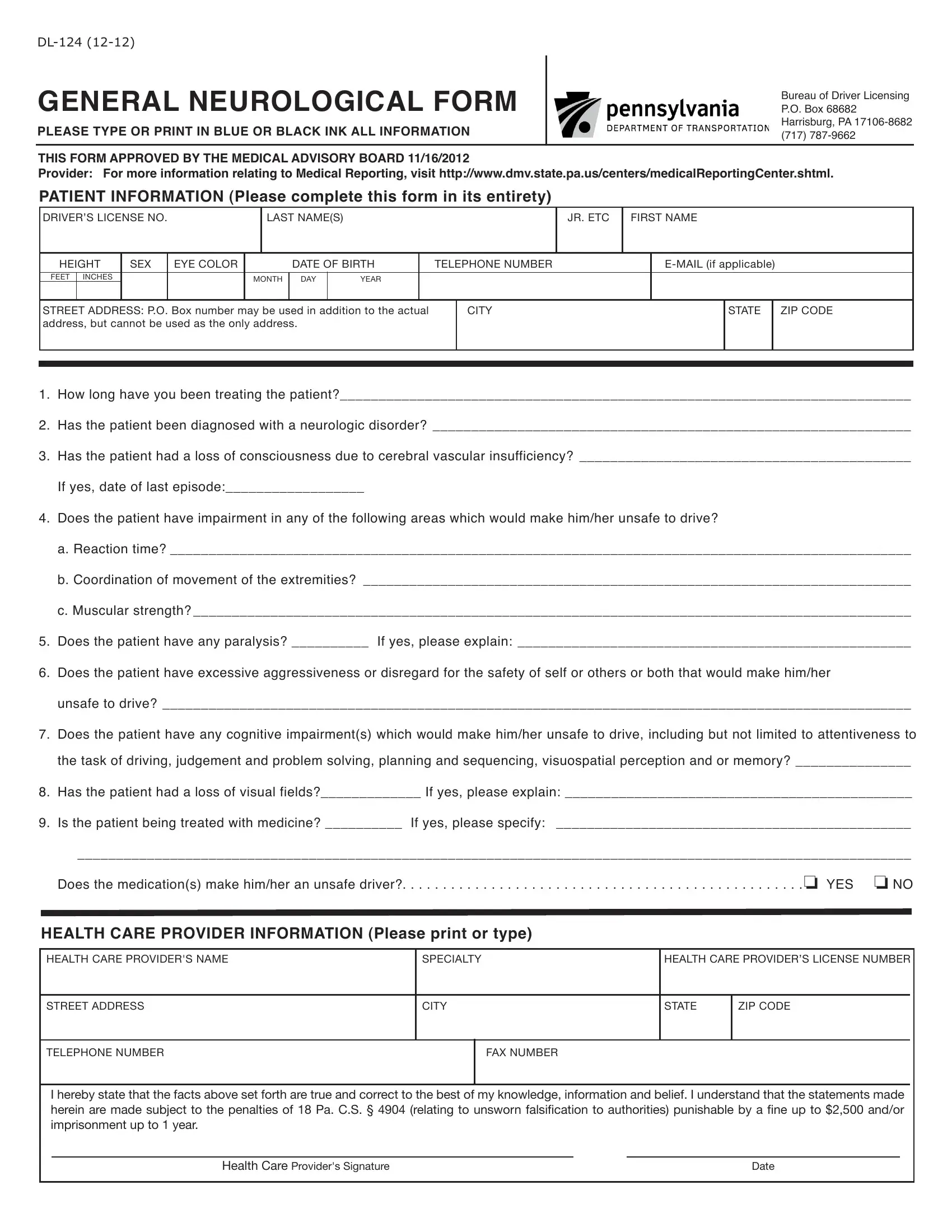
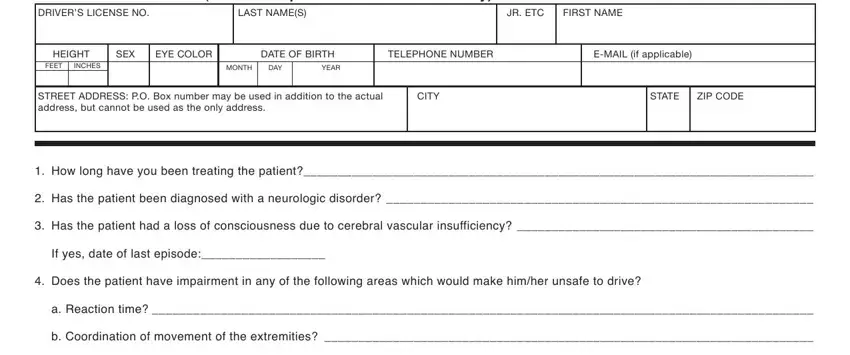
1. For starters, once filling in the pennsylvania 124 form, start in the form section that features the following blanks:
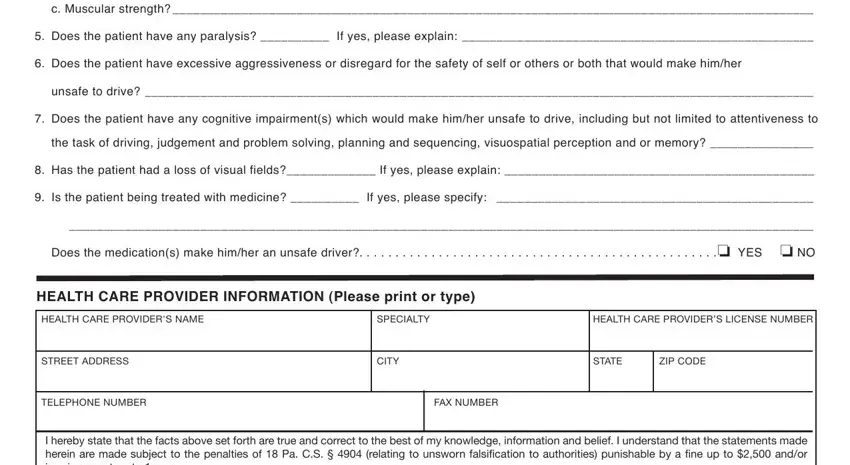
2. The third stage would be to submit these fields: c Muscular strength, Does the patient have any, Does the patient have excessive, unsafe to drive, Does the patient have any, the task of driving judgement and, Has the patient had a loss of, Is the patient being treated with, Does the medications make himher, HEALTH CARE PROVIDER INFORMATION, HEALTH CARE PROVIDERS NAME, SPECIALTY, HEALTH CARE PROVIDERS LICENSE, STREET ADDRESS, and CITY.
Always be extremely attentive when filling out HEALTH CARE PROVIDERS NAME and SPECIALTY, because this is where a lot of people make some mistakes.
3. This subsequent part is usually quite straightforward, I hereby state that the facts, Health Care Providers Signature, and Date - these fields will have to be completed here.

Step 3: Be certain that your information is accurate and then press "Done" to complete the task. Try a 7-day free trial subscription with us and obtain instant access to pennsylvania 124 form - downloadable, emailable, and editable in your FormsPal account. With FormsPal, you're able to fill out documents without worrying about data breaches or records getting shared. Our protected software ensures that your private information is kept safe.