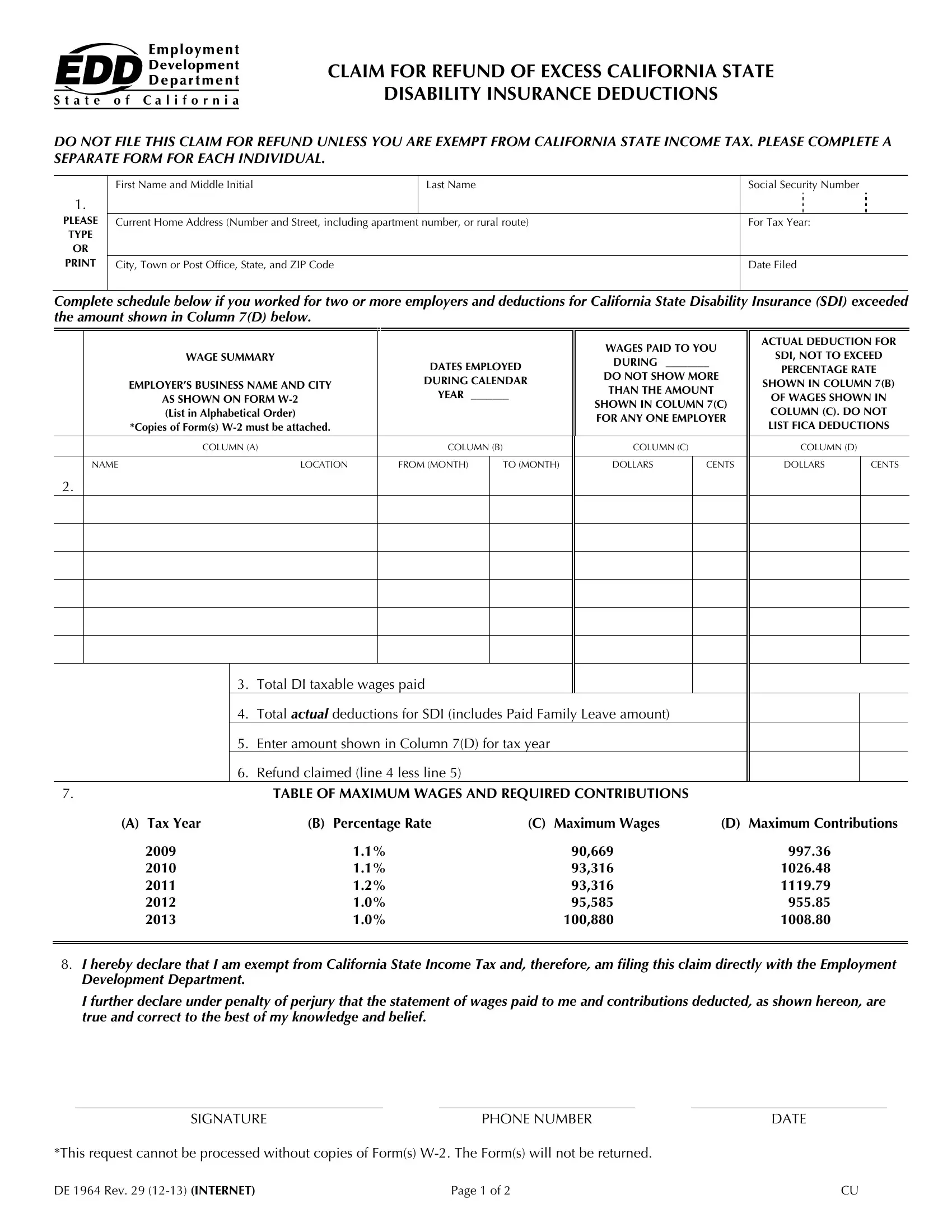
Navigating the complexities of tax and insurance deductions can often feel like a maze, and the Edd De form, officially known as the Claim for Refund of Excess California State Disability Insurance Deductions, serves as a beacon for individuals who find themselves overpaying on their state disability insurance (SDI). Exclusively applicable to those exempt from California State Income Tax, this form provides a streamlined process for claiming a refund on excess SDI deductions. To initiate a claim, individuals must provide detailed personal information, include their employment and earnings history, and attach pertinent documents such as copies of their Form(s) W-2. It's essential to carefully document wages from multiple employers, ensuring that the total SDI deductions do not exceed the statutory threshold established for the given tax year. The guidelines stipulate that claims must be based on calendar year wages only and must be filed within a three-year period following the calendar year in which the excess deductions occurred. Moreover, clear instructions are provided regarding the specific conditions under which wages are eligible for consideration within a claim. The intricacies of the DE 1964 form highlight the importance of meticulousness and accuracy in pursuing a refund, emphasizing its role as a critical tool for those eligible to navigate their way to reclaiming excess deductions rightfully theirs.
| Question | Answer |
|---|---|
| Form Name | Edd Form De 1964 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | de1964 edd 1964 form |
