
With the online PDF editor by FormsPal, you can complete or change benefit enrollment form template here and now. In order to make our tool better and simpler to use, we consistently work on new features, with our users' suggestions in mind. Starting is simple! Everything you need to do is follow the next easy steps down below:
Step 1: Open the form inside our tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: The tool offers you the opportunity to customize most PDF forms in a range of ways. Transform it by adding customized text, adjust original content, and include a signature - all at your fingertips!
It really is an easy task to complete the document using out detailed tutorial! Here is what you want to do:
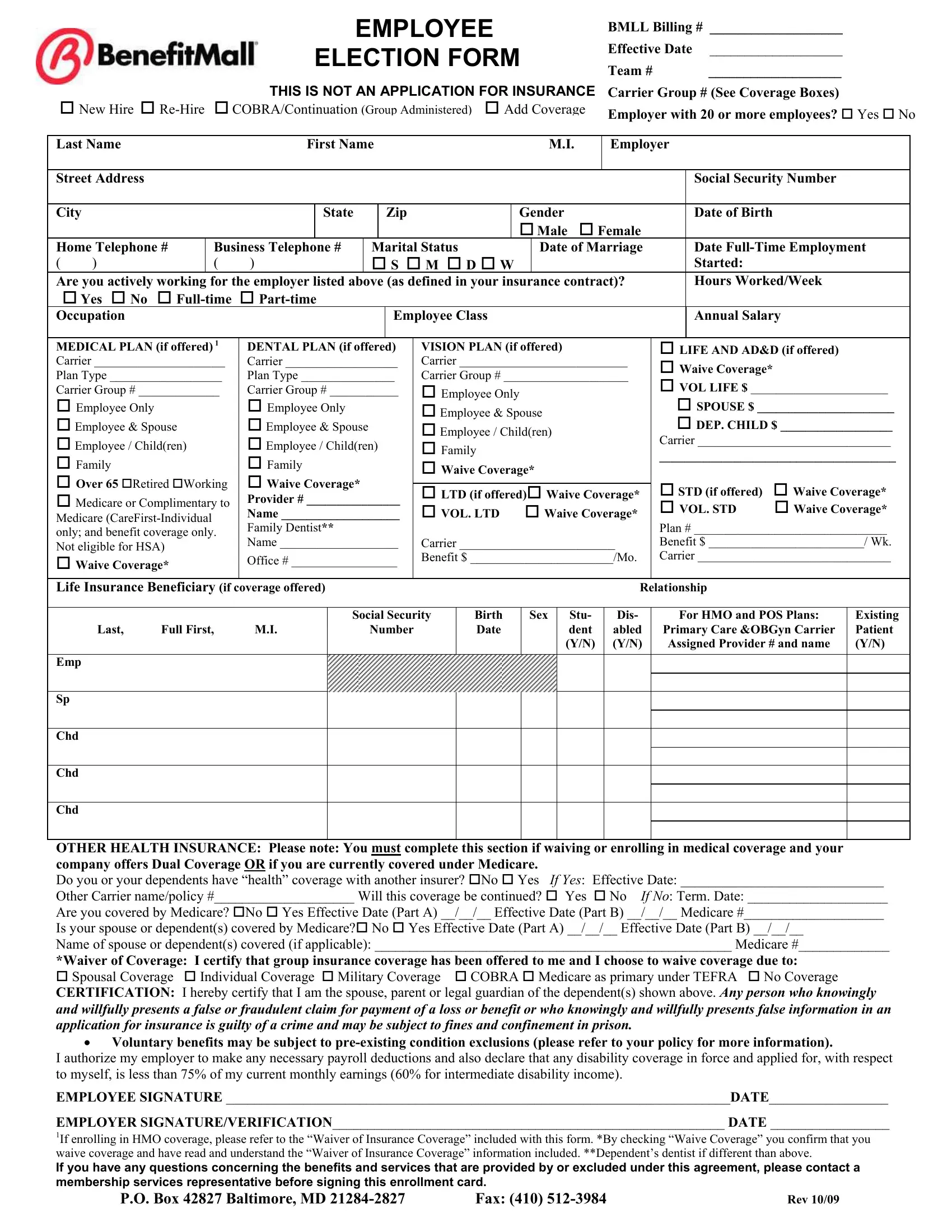
1. You should complete the benefit enrollment form template properly, therefore take care while filling in the parts comprising these specific fields:
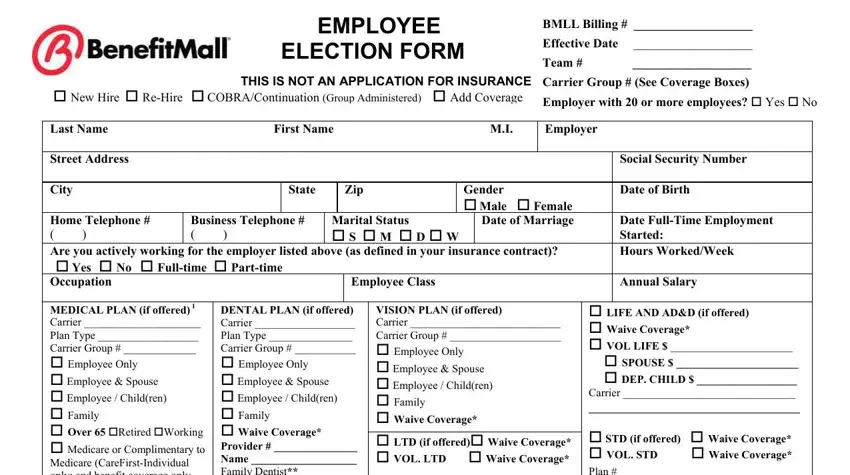
2. Soon after finishing this part, go on to the next stage and complete all required details in these blanks - MEDICAL PLAN if offered Carrier, DENTAL PLAN if offered Carrier, Office, VISION PLAN if offered Carrier, cid LIFE AND ADD if offered cid, Life Insurance Beneficiary if, Last Full First MI, Social Security, Number, Birth Date, Sex, Stu dent YN, Dis abled YN, For HMO and POS Plans, and Primary Care OBGyn Carrier.
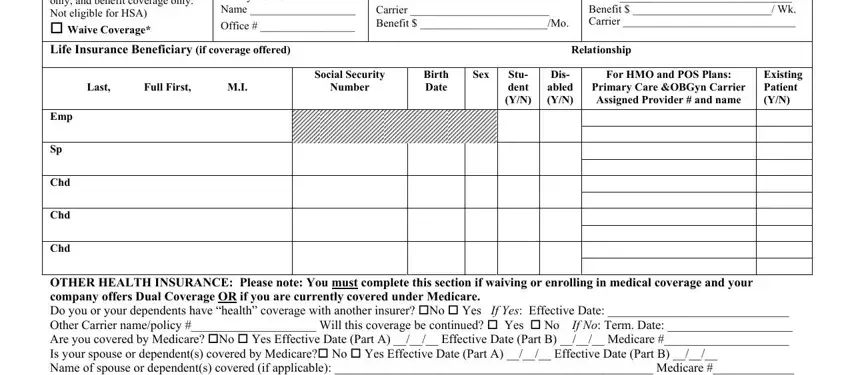
Concerning Stu dent YN and Primary Care OBGyn Carrier, make sure that you review things in this section. Those two are surely the most significant fields in the PDF.
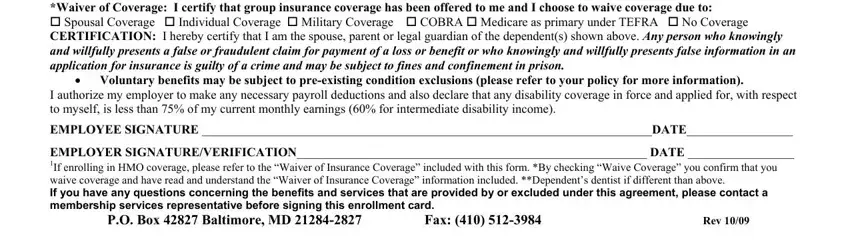
3. This next part is considered pretty straightforward, OTHER HEALTH INSURANCE Please note, Voluntary benefits may be subject, I authorize my employer to make, EMPLOYEE SIGNATURE DATE, EMPLOYER SIGNATUREVERIFICATION, PO Box Baltimore MD Fax, and Rev - these empty fields will need to be filled in here.
Step 3: Prior to addressing the next stage, you should make sure that blank fields have been filled in properly. Once you confirm that it is correct, press “Done." Get hold of your benefit enrollment form template when you join for a 7-day free trial. Immediately gain access to the pdf file from your FormsPal account page, with any modifications and changes being all synced! We do not share any details you enter whenever completing forms at FormsPal.