The filling out the dwc 1 florida is actually quick. Our team ensured our software is not difficult to work with and helps complete any sort of form in no time. Take a look at a couple of steps you'll want to take:
Step 1: Press the "Get Form Now" button to start out.
Step 2: Now you will be within the form edit page. You can add, transform, highlight, check, cross, include or erase fields or text.
Type in the content requested by the application to prepare the document.
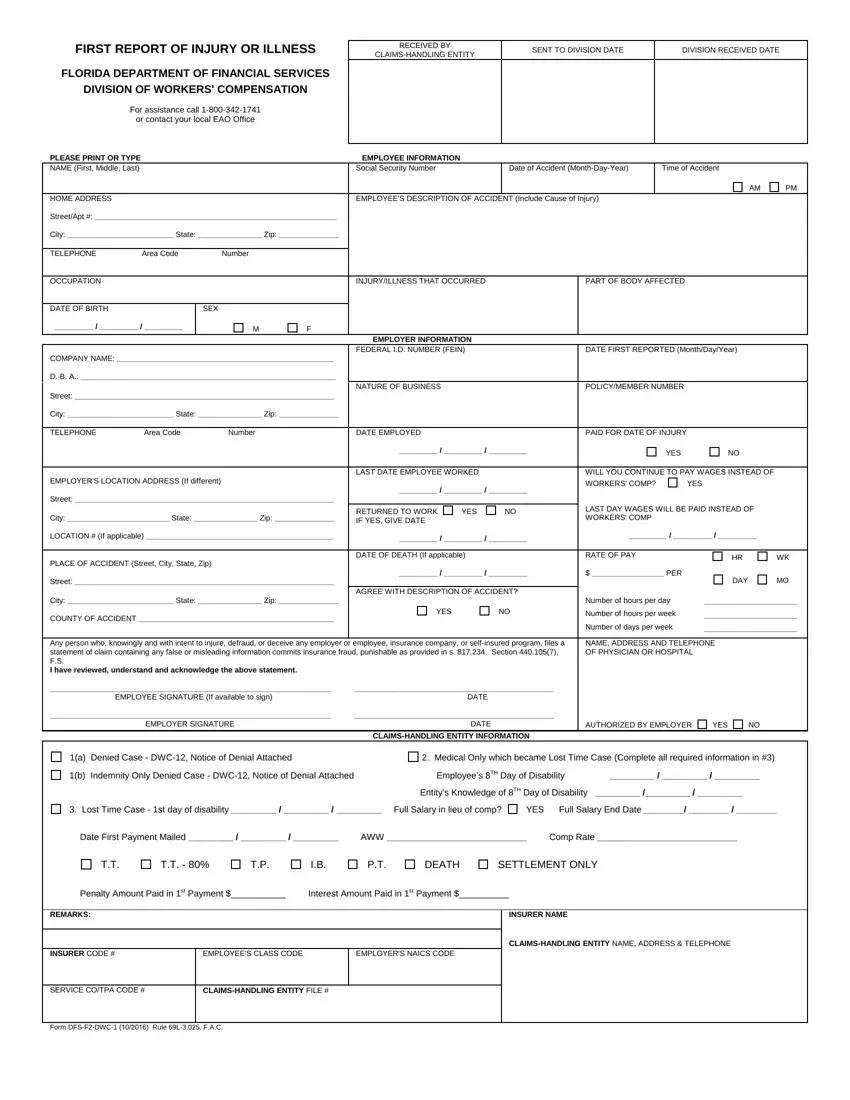
Include the essential details in the Street, City State Zip, TELEPHONE, Area Code, Number, DATE EMPLOYED, PAID FOR DATE OF INJURY, YES, EMPLOYERS LOCATION ADDRESS If, Street, City State Zip, LAST DATE EMPLOYEE WORKED, WILL YOU CONTINUE TO PAY WAGES, YES, and RETURNED TO WORK IF YES GIVE DATE segment.
In the b Indemnity Only Denied Case DWC, Employees TH Day of Disability, Entitys Knowledge of TH Day of, Lost Time Case st day of, YES Full Salary End Date, Date First Payment Mailed AWW, DEATH, SETTLEMENT ONLY, Penalty Amount Paid in st Payment, REMARKS, INSURER NAME, INSURER CODE, EMPLOYEES CLASS CODE, EMPLOYERS NAICS CODE, and CLAIMSHANDLING ENTITY NAME ADDRESS segment, point out the crucial information.
Step 3: Hit the Done button to save the document. At this point it is ready for upload to your gadget.
Step 4: Try to create as many duplicates of your form as you can to keep away from potential problems.
