We were building the PDF editor having the idea of making it as simple make use of as possible. That's the reason the procedure of typing in the printable 1010 form will likely to be simple accomplish all of these steps:
Step 1: Locate the button "Get Form Here" and then click it.
Step 2: As soon as you have accessed your printable 1010 form edit page, you'll discover all functions you may use regarding your file in the top menu.
Provide the data demanded by the application to prepare the form.
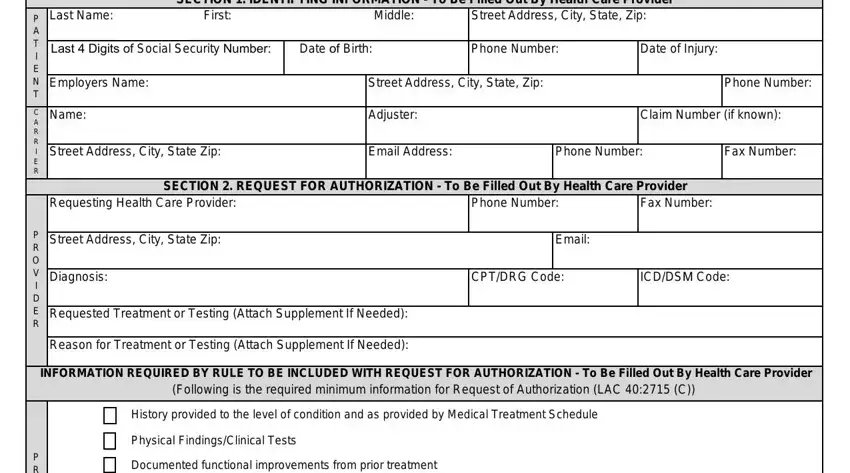
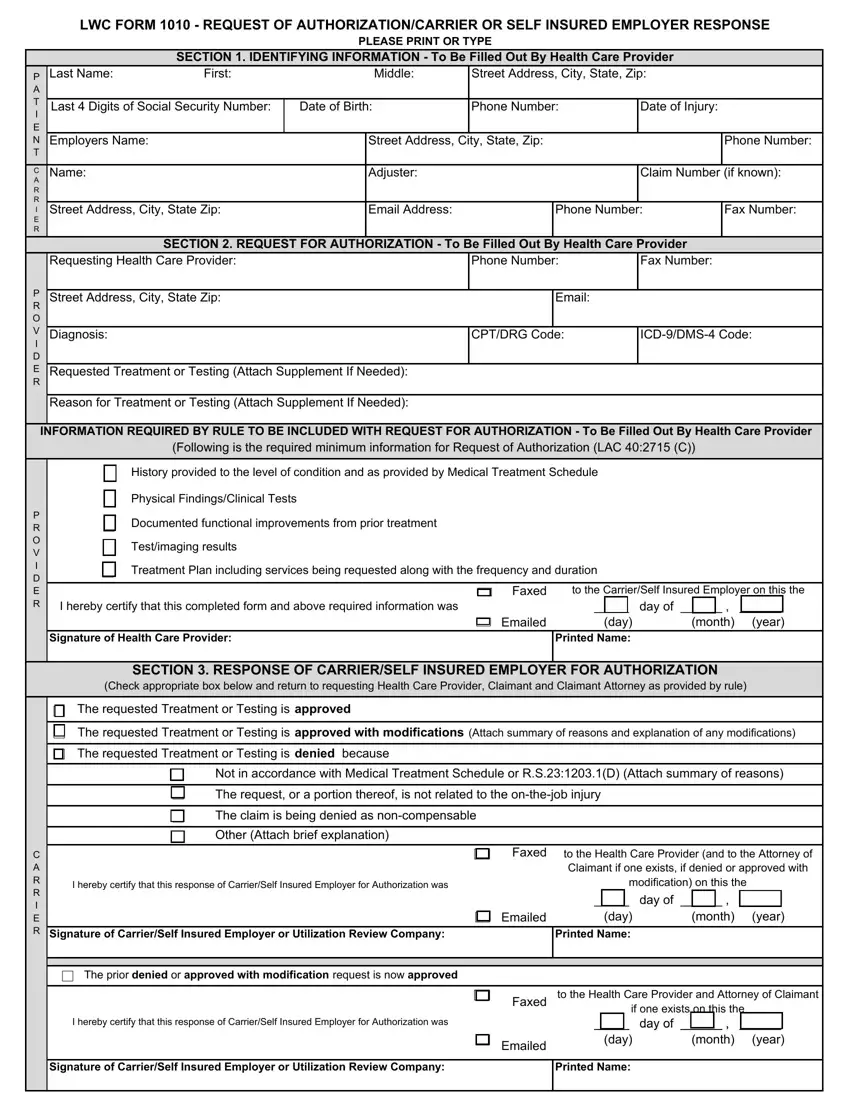
Complete the P P R O V I D E R, C A R R I E R, Testimaging results, Treatment Plan including services, I hereby certify that this, Signature of Health Care Provider, Faxed, Emailed, to the CarrierSelf Insured, SECTION RESPONSE OF CARRIERSELF, The requested Treatment or Testing, The requested Treatment or Testing, The requested Treatment or Testing, Not in accordance with Medical, and The request or a portion thereof fields with any content which may be demanded by the system.
In the C A R R I E R, Signature of CarrierSelf Insured, The prior denied or approved with, I hereby certify that this, p y, Emailed, day of month year, day Printed Name, Faxed, Emailed, to the Health Care Provider and, Signature of CarrierSelf Insured, and Printed Name area, focus on the essential data.
The Form A is required to be filled, The requested Treatment or Testing, I hereby certify that this First, Signature of CarrierSelf Insured, Faxed, Emailed, to the Health Care Provider on, I hereby certify that a response, Signature of Health Care Provider, Faxed, to the CarrierSelf Insured, Emailed, day of day month year Printed, SECTION SUSPENSION OF PRIOR, and Suspension of Prior Authorization area enables you to point out the rights and responsibilities of either side.
End by looking at the following fields and filling them in as required: I hereby certify that this form, I hereby certify that this Appeal, Faxed, to the CarrierSelf Insured, Signature of Health Care Provider, Printed Name, SECTION DETERMINATION OF MEDICAL, The required information of LACC, The required information of LACC, I hereby certify that a written, Signature, Faxed, to the Health Care Provider, Emailed, and day of month year.
Step 3: As you hit the Done button, your ready file is easily exportable to any type of of your gadgets. Or, you might send it using mail.
Step 4: Generate copies of the document. It will save you from upcoming problems. We don't look at or disclose your details, therefore you can relax knowing it's going to be secure.
