
Using the online tool for PDF editing by FormsPal, you can fill in or edit Form 11318 right here and now. Our editor is constantly developing to grant the best user experience achievable, and that's thanks to our commitment to continual improvement and listening closely to user comments. By taking a few basic steps, it is possible to start your PDF editing:
Step 1: Press the orange "Get Form" button above. It is going to open up our tool so that you can start completing your form.
Step 2: The editor lets you change nearly all PDF documents in various ways. Enhance it with customized text, correct existing content, and place in a signature - all close at hand!
This form requires specific details; to guarantee consistency, you need to take into account the suggestions just below:
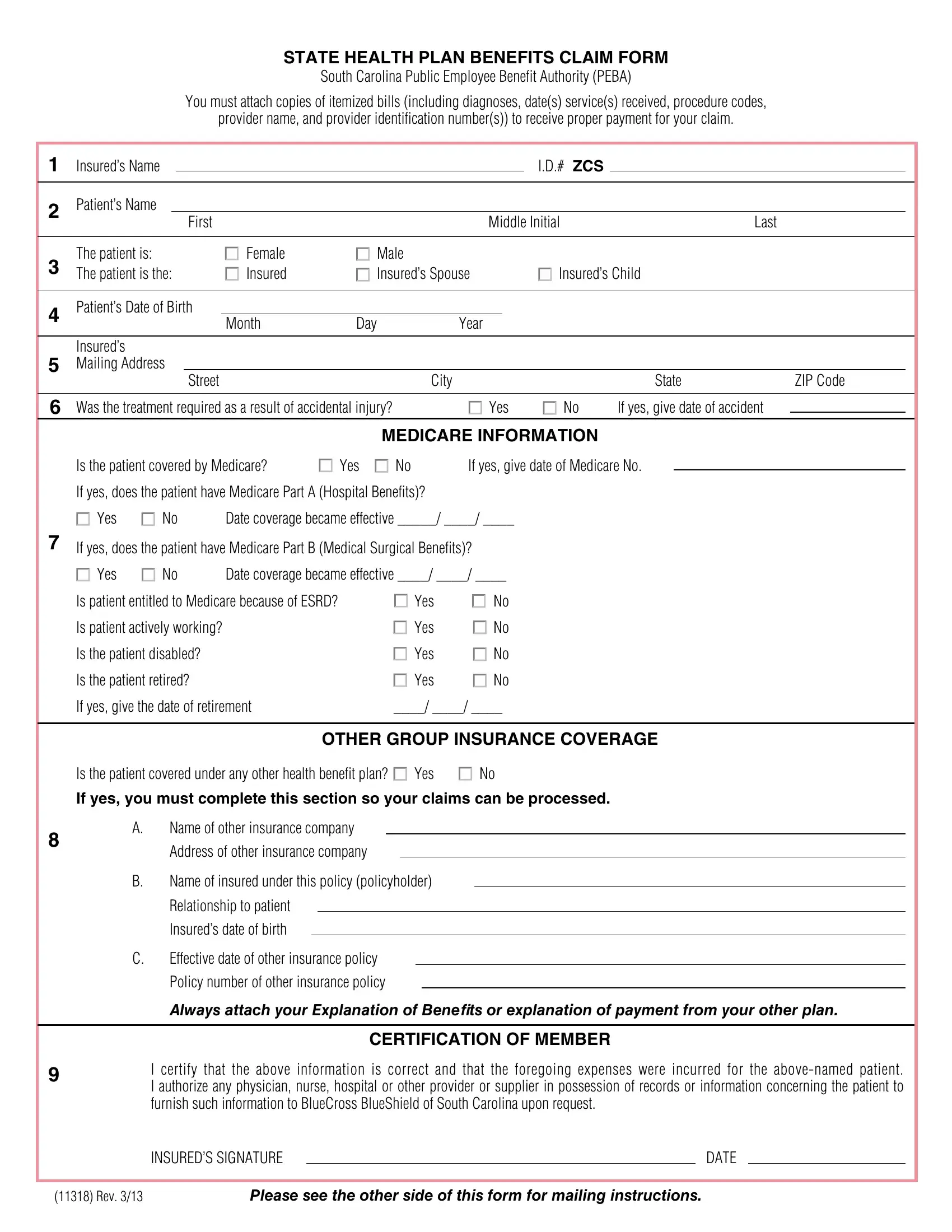
1. Fill out your Form 11318 with a selection of necessary blank fields. Collect all of the information you need and ensure there's nothing forgotten!
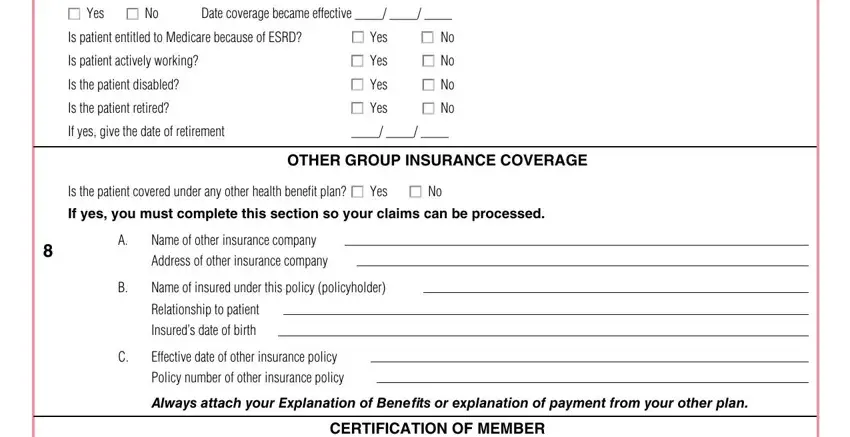
2. Right after finishing this part, go to the next stage and complete the necessary details in these blank fields - M Yes M No, Date coverage became effective, Is patient entitled to Medicare, Is patient actively working, Is the patient disabled, Is the patient retired, M Yes, M Yes, M Yes, M Yes, M No, M No, M No, M No, and If yes give the date of retirement.
3. Completing INSUREDS SIGNATURE, DATE, Rev, and Please see the other side of this is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Always be extremely careful while completing DATE and Please see the other side of this, as this is where many people make errors.
Step 3: When you have reread the information in the fields, simply click "Done" to finalize your document generation. Join us today and instantly obtain Form 11318, all set for downloading. Every modification you make is conveniently kept , which enables you to edit the form later on if required. FormsPal is focused on the confidentiality of all our users; we make certain that all information handled by our editor stays confidential.