






You can certainly get forms taking advantage of our PDF editor. Revising the allianz forms form is effortless in case you use the next actions:
Step 1: Select the button "Get Form Here" on the webpage and select it.
Step 2: At this point, you're on the form editing page. You may add information, edit existing details, highlight certain words or phrases, put crosses or checks, insert images, sign the form, erase needless fields, etc.
These particular segments will compose the PDF form that you will be filling in:
You should note your data within the field Option Payment to policyholder, Preferred payment method, Bank transfer, Cheque, Please specify the currency you, Name of bank account holder as, Account number, IBAN where required, Sortbranch code, Name of bank, Bank address, BICSwift code, If you are aware of any additional, Swift code of intermediary bank, and For bank transfer please provide.
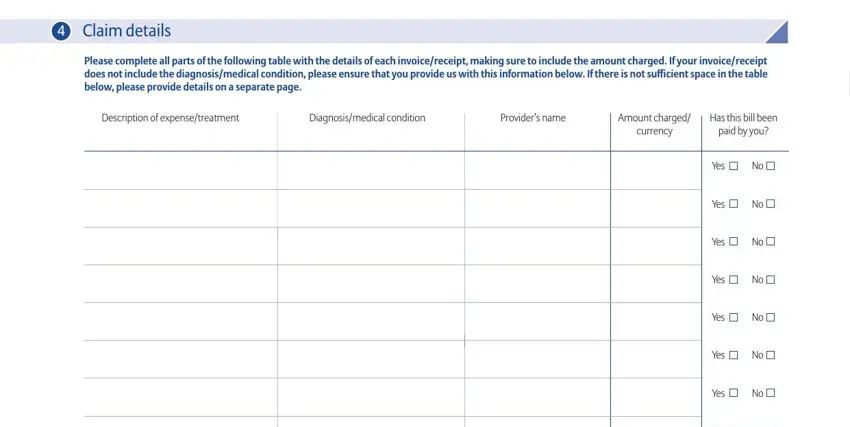
The system will require for more info to quickly fill in the part Claim details, Please complete all parts of the, Description of expensetreatment, Diagnosismedical condition, Providers name, Amount charged currency, Has this bill been paid by you, Yes, Yes, Yes, Yes, Yes, Yes, Yes, and Yes.
The Yes, Yes, Yes, Yes, Yes, Yes, Yes, Yes, Yes, Yes, Yes, and Yes box will be your place to put the rights and responsibilities of all sides.
End by taking a look at the following sections and filling them in as needed: Yes, In what country did the treatment, Has preauthorization been obtained, Yes, cid, and If this claim is resulting from an.
Step 3: When you are done, hit the "Done" button to export the PDF document.
Step 4: Make a minimum of a couple of copies of your document to avoid any specific upcoming problems.
