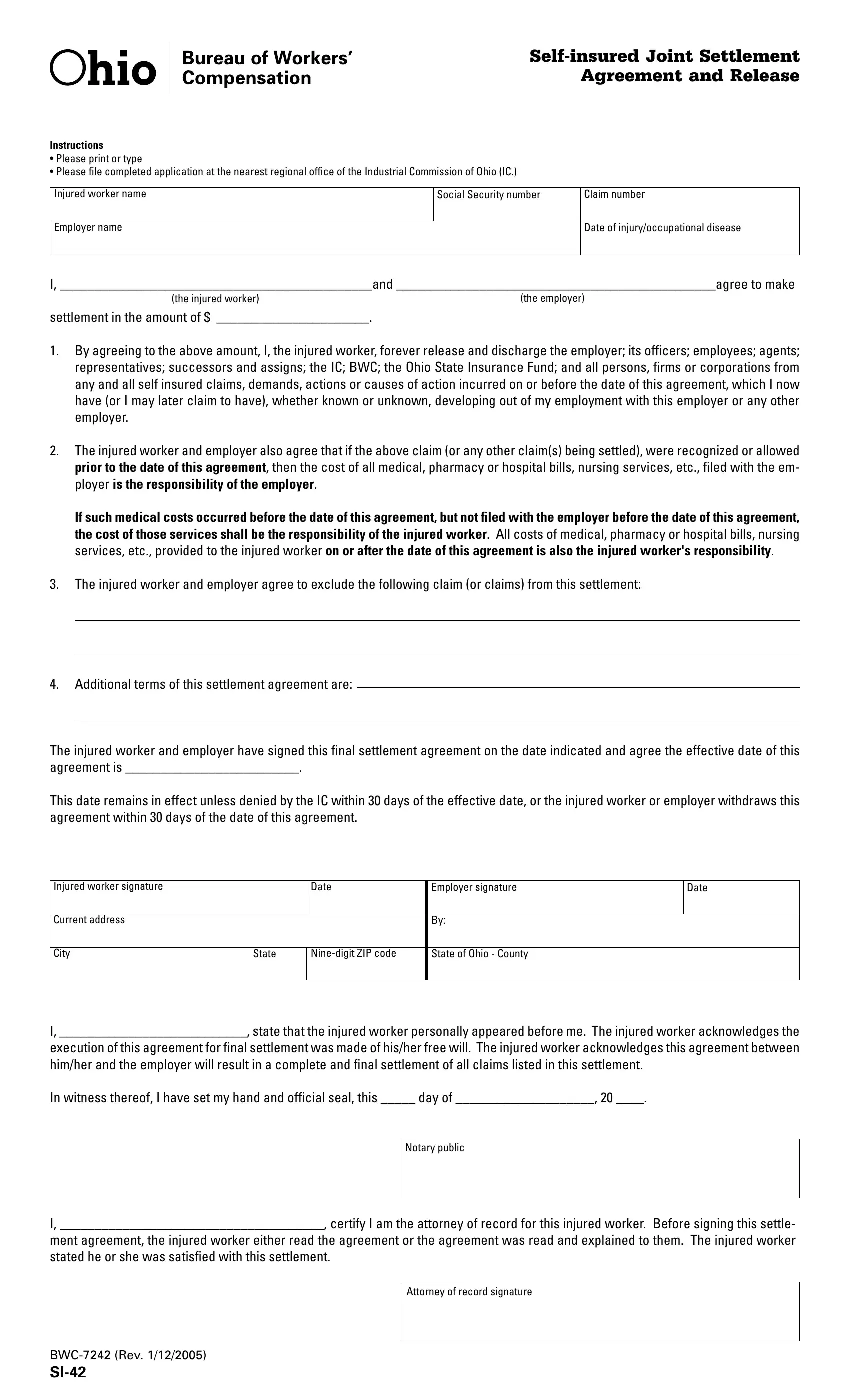
Navigating the complexities of workers' compensation settlements requires a thorough understanding of the necessary paperwork, one of the key documents being the BWC 7242 form, officially known as the Self-insured Joint Settlement Agreement and Release. This form serves as a crucial agreement between an injured worker and their employer to resolve any claims related to workplace injuries or occupational diseases without further disputes. It requires comprehensive details such as the injured worker's name, social security number, claim number, and specific information about the employer alongside the date of the injury or disease. At its core, the form establishes an agreed sum for settlement, marking the injured party's agreement to release the employer and associated entities from any further claims or actions related to the injury up to the agreement's date. Uniquely, the form also clarifies responsibilities for medical costs incurred before and after the agreement's effective date and allows for the exclusion of specific claims from the settlement. Additionally, it outlines the process for the agreement's effectiveness, subject to the Industrial Commission of Ohio’s approval, and specifies the roles of witnesses, including a notary public and the injured worker's attorney, to affirm the agreement's legitimacy and voluntary nature. Understanding the nuances and stipulations of this form is crucial for both parties to ensure a fair and final resolution of workers' compensation claims.
| Question | Answer |
|---|---|
| Form Name | Form Bwc 7242 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | assigns, digit, BWC, si 42 fillable |
Agreement and Release
Instructions
•Please print or type
•Please ile completed application at the nearest regional ofice of the Industrial Commission of Ohio (IC.)
Injured worker name
Social Security number
Claim number
Employer name
Date of injury/occupational disease
I, _____________________________________________and ______________________________________________agree to make
(the injured worker) |
(the employer) |
settlement in the amount of $ ______________________. |
|
1.By agreeing to the above amount, I, the injured worker, forever release and discharge the employer; its oficers; employees; agents; representatives; successors and assigns; the IC; BWC; the Ohio State Insurance Fund; and all persons, irms or corporations from any and all self insured claims, demands, actions or causes of action incurred on or before the date of this agreement, which I now have (or I may later claim to have), whether known or unknown, developing out of my employment with this employer or any other employer.
2.The injured worker and employer also agree that if the above claim (or any other claim(s) being settled), were recognized or allowed prior to the date of this agreement, then the cost of all medical, pharmacy or hospital bills, nursing services, etc., iled with the em- ployer is the responsibility of the employer.
If such medical costs occurred before the date of this agreement, but not filed with the employer before the date of this agreement, the cost of those services shall be the responsibility of the injured worker. All costs of medical, pharmacy or hospital bills, nursing services, etc., provided to the injured worker on or after the date of this agreement is also the injured worker's responsibility.
3.The injured worker and employer agree to exclude the following claim (or claims) from this settlement:
4.Additional terms of this settlement agreement are:
The injured worker and employer have signed this inal settlement agreement on the date indicated and agree the effective date of this agreement is _________________________.
This date remains in effect unless denied by the IC within 30 days of the effective date, or the injured worker or employer withdraws this agreement within 30 days of the date of this agreement.
Injured worker signature |
|
Date |
Employer signature |
Date |
|
|
|
|
|
Current address |
|
|
By: |
|
|
|
|
|
|
City |
State |
State of Ohio - County |
|
|
|
|
|
|
|
I, ___________________________, state that the injured worker personally appeared before me. The injured worker acknowledges the
execution of this agreement for inal settlement was made of his/her free will. The injured worker acknowledges this agreement between him/her and the employer will result in a complete and inal settlement of all claims listed in this settlement.
In witness thereof, I have set my hand and oficial seal, this _____ day of ____________________, 20 ____.
Notary public
I, ______________________________________, certify I am the attorney of record for this injured worker. Before signing this settle-
ment agreement, the injured worker either read the agreement or the agreement was read and explained to them. The injured worker stated he or she was satisied with this settlement.
Attorney of record signature