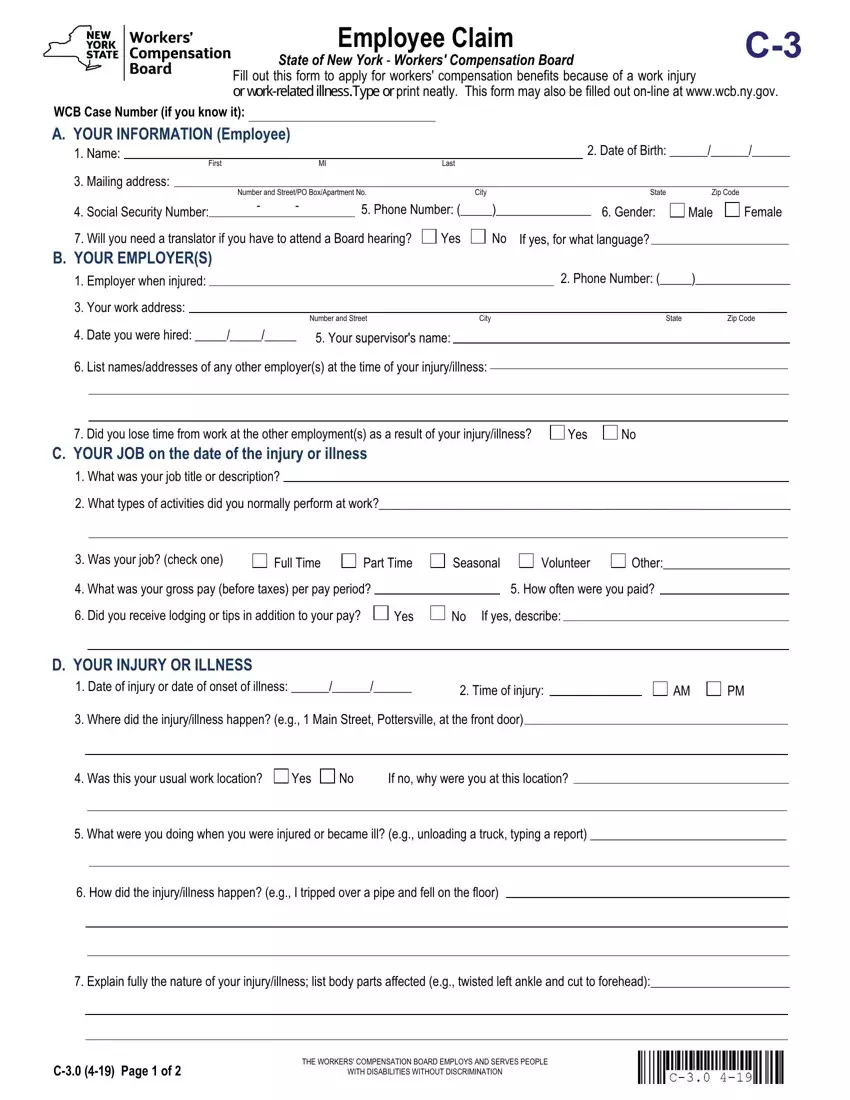
Instructions for Completing Employee Claim (Form C-3)
Please complete this form and send it to the Workers' Compensation Board centralized mailing address listed at the end of these instructions. If you need additional help completing this form, contact the Workers' Compensation Board at 1-877-632-4996. You may also fill this form out online at wcb.ny.gov. If you do not have or know your Workers' Compensation Board Case Number, please leave this field blank. It is not required to process your claim. Remember to enter your name and the date of your injury/illness on the top of page two.
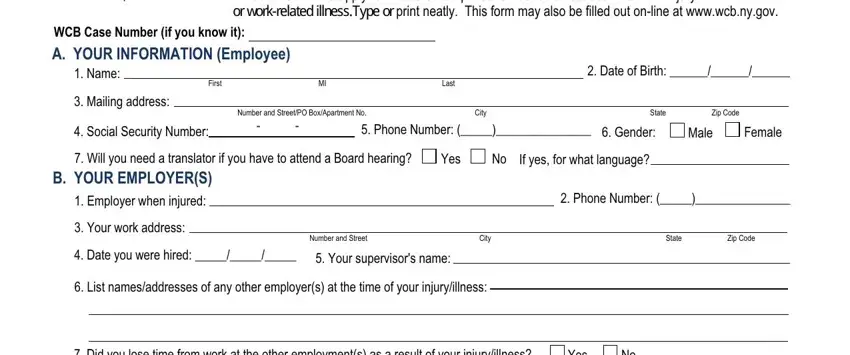
Section A - Your Information (Employee):
In Section A, enter your name, address and other requested information.
Note on Item 7: Board hearings are conducted in English. If you need a translator, select Yes and indicate the language needed.
Notification Pursuant to the New York Personal Privacy Protection Law
(Public Officers Law Article 6-A) and the Federal Privacy Act of 1974 (5 U.S.C. § 552a).
The Workers' Compensation Board's (Board’s) authority to request that claimants provide personal information, including their social security number, is derived from the Board’s investigatory authority under Workers' Compensation Law (WCL) § 20, and its administrative authority under WCL § 142. This information is collected to assist the Board in investigating and administering claims in the most expedient manner possible and to help it maintain accurate claim records. Providing your social security number to the Board is voluntary. There is no penalty for failure to provide your social security number on this form; it will not result in a denial of your claim or a reduction in benefits. The Board will protect the confidentiality of all personal information in its possession, disclosing it only in furtherance of its official duties and in accordance with applicable state and federal law.
Section B - Your Employer(s):
In Section B, enter the name, address, phone number and other information of the employer you were working for at the time of the injury/illness.
Note: Your employer is the company or agency that issues your paycheck. If you are a contractor at a work site or office, the staffing agency or vendor who hired you is your employer, not the work site or office where you report to work.
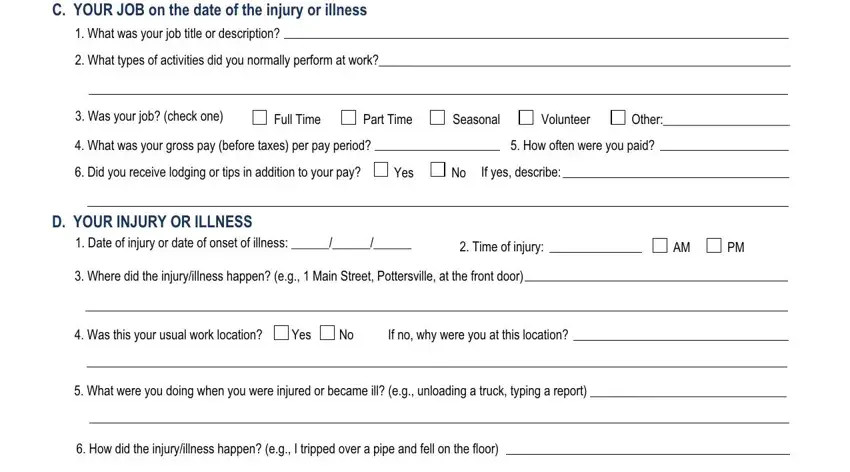
Section C - Your Job on the Date of the Injury or Illness:
In Section C, enter your job title, work activities and pay information.
Section D - Your Injury or Illness:
In Section D, enter your injury or illness information.
Item 1: Enter the date you were injured or the first date you noticed you became ill.
If this is an illness or occupational disease, skip item 2. The date you were injured must be in month/day/year format. The year should be written as four digits, e.g., 2015.
Item 2: Enter the time when the injury occurred. Check whether it was AM or PM.
Item 3: Indicate the location where the injury/illness occurred, including the address of the building and the physical location in the building where the injury/illness happened.
Item 4: Check whether this was your normal work location. If it was not, explain why you were at this location.
Item 5: Describe in detail what you were doing at the time of the injury/illness (e.g., unloading boxes from a truck by hand). This explains the events leading up to the injury.
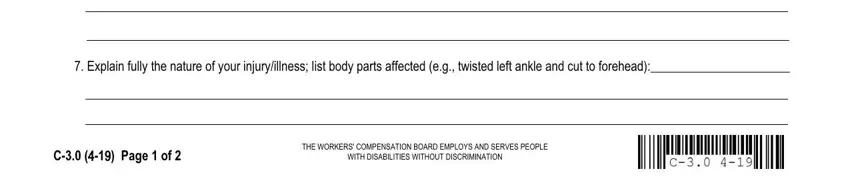
Item 6: Describe in detail how the injury/illness occurred (e.g., I was lifting a heavy box off a truck). This should include all people and events involved in the injury/illness.
Item 7: Indicate fully the nature and extent of your injury/illness, including all body parts injured. Be as specific as possible (e.g., I strained my back trying to lift a heavy box. It hurts to bend over or hold even lighter objects now).
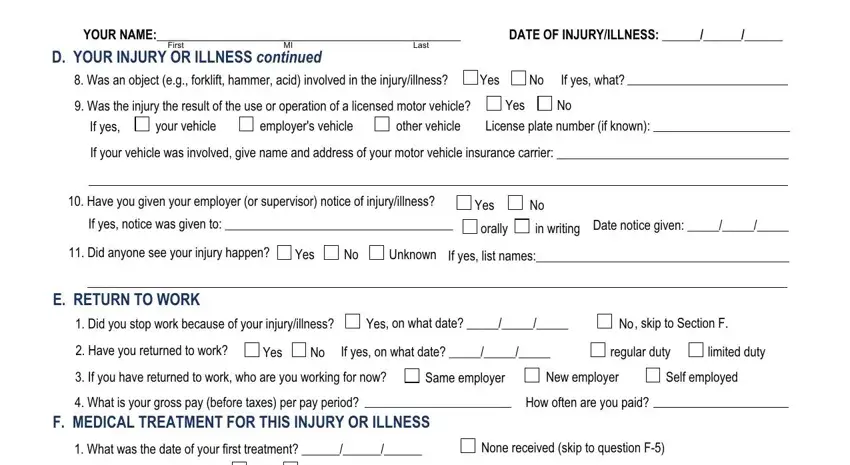
Item 8: Indicate if some object was involved in the accident other than a licensed motor vehicle. Other objects may include a tool (e.g., hammer), a chemical (e.g., acid), machinery (e.g., forklift or drill press), etc.
Item 9: Indicate if a licensed motor vehicle was involved in the accident. If so, check if the motor vehicle involved was yours, your employer's, or a third party's. Include the license plate number (if known). If your vehicle was involved, fill out the name and address of your automobile liability insurance carrier.
Item 10: Check if you gave your employer or supervisor notice of your injury or illness. If so, indicate who you gave notice to as well as if it was orally or in writing. Include the date you gave notice.
Item 11: Check if anyone else saw the injury happen. If anyone did see it, include their name(s).
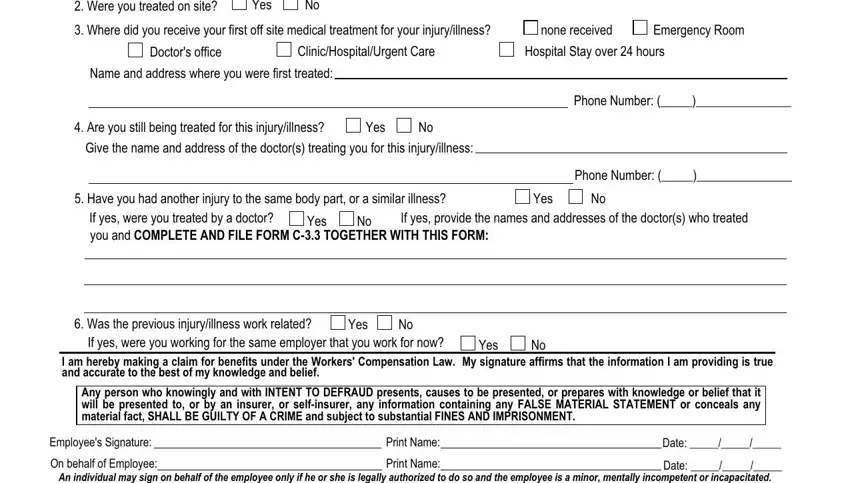
Section E - Return to Work:
Item 1: If you stopped working as a result of your work-related injury/illness, check Yes and indicate the date you stopped working. If you have not stopped working, check No and skip to the next section.
Item 2: If you have since returned to work, check Yes. Also indicate on what date you started working again, as well as if you have returned to your Normal Duties or if you are on Limited or Restricted Duty. (If you have not returned to your full pre-injury or illness work duties, then you are on Limited Duty.)
Item 3: If you have returned to work, indicate who you are working for now.
Item 4: Enter your gross pay (before tax pay) per pay period for the job you are working at now. Indicate how often you are receiving a paycheck (weekly, bi-weekly, etc.).

 Yes
Yes 
 No If yes, for what language?
No If yes, for what language?






 Psychotherapy notes
Psychotherapy notes Alcohol/Drug treatment
Alcohol/Drug treatment Mental Health treatment
Mental Health treatment 





 Información relacionada con el VIH
Información relacionada con el VIH Notas de terapia psicológica
Notas de terapia psicológica Tratamientos por abuso de alcohol o drogas
Tratamientos por abuso de alcohol o drogas Tratamiento de salud mental
Tratamiento de salud mental