Our PDF editor was made to be as simple as it can be. As soon as you follow the following steps, the process of completing the health form necessity form will be easy.
Step 1: The first thing would be to click the orange "Get Form Now" button.
Step 2: You can now edit your health form necessity. The multifunctional toolbar helps you include, eliminate, modify, and highlight text as well as carry out other sorts of commands.
To be able to prepare the template, enter the details the system will require you to for each of the next segments:
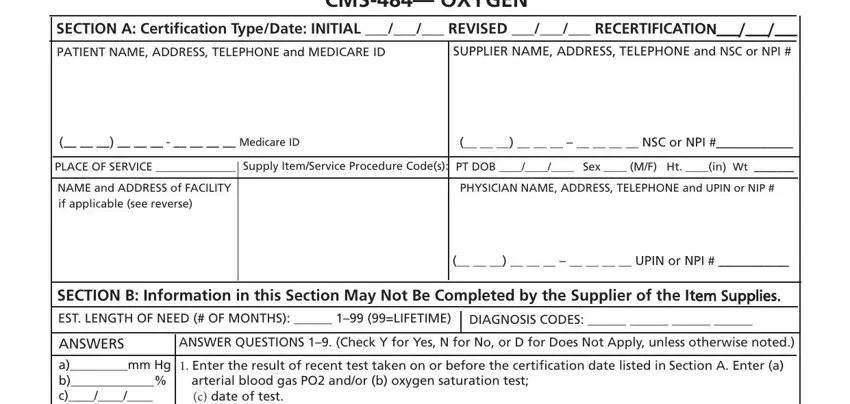
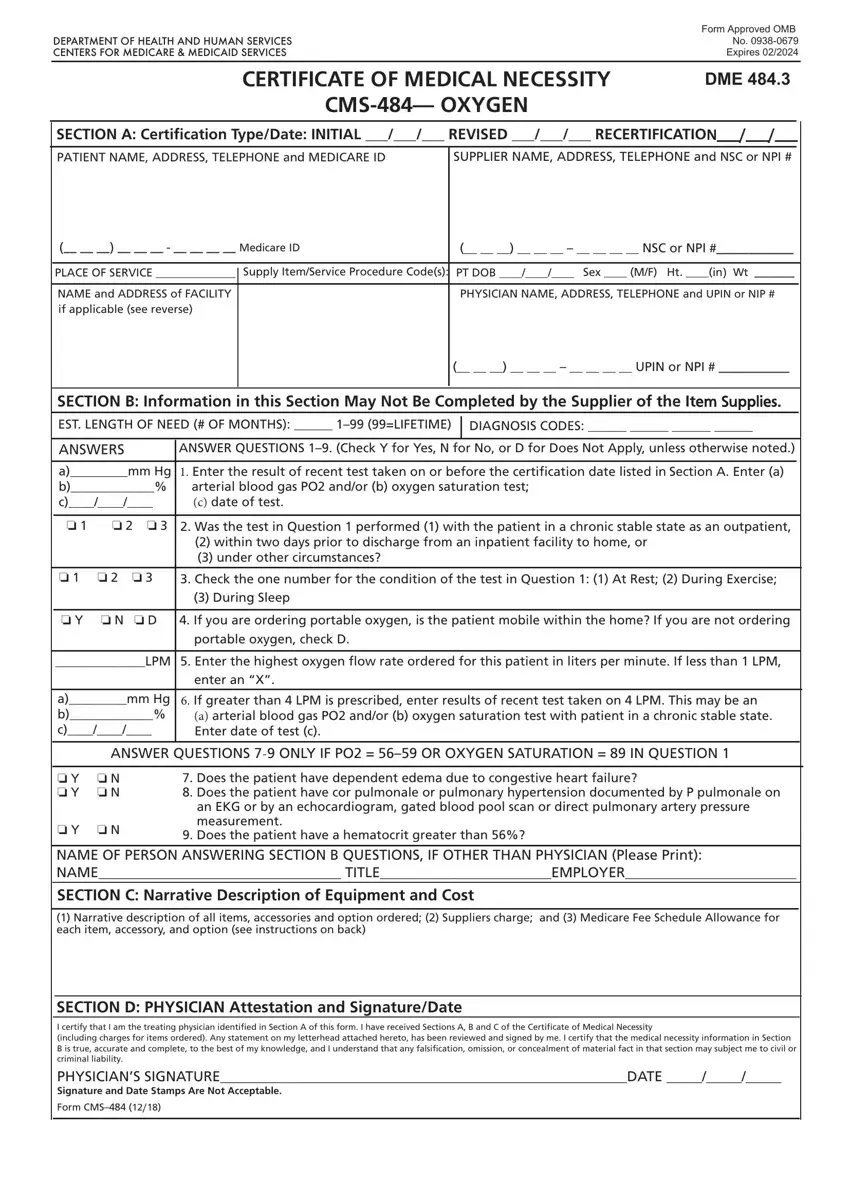
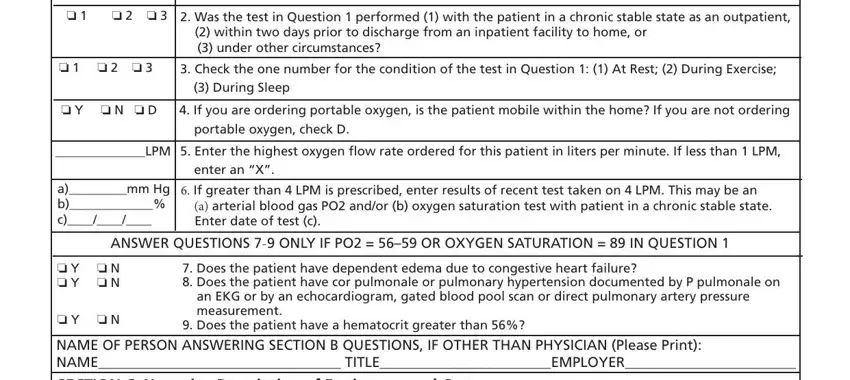
You need to write your information in the part arterial blood gas PO andor b, o o Was the test in Question, within two days prior to, o o o, Check the one number for the, During Sleep, o Y o N o D, If you are ordering portable, portable oxygen check D, LPM Enter the highest oxygen fow, enter an X, amm Hg b c, If greater than LPM is, a arterial blood gas PO andor b, and ANSWER QUESTIONS ONLY IF PO OR.
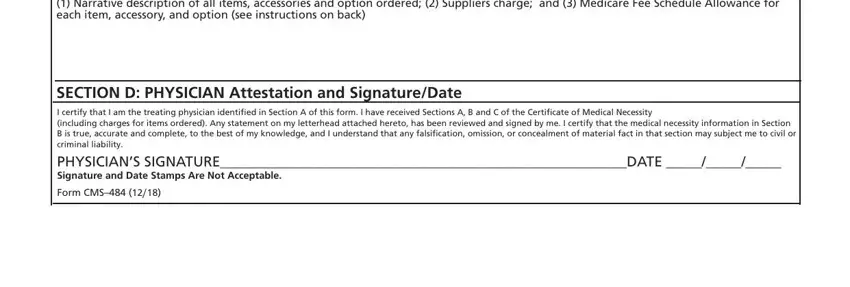
You need to emphasize the fundamental information from the Narrative description of all, SECTION D PHYSICIAN Attestation, and Form CMS field.
The area According to the Paperwork, DO NOT SuBMIT CLAIMS TO THIS, and Form CMS INSTRUCTIONS should be where one can include all sides' rights and obligations.

Step 3: After you click the Done button, your finalized document may be transferred to each of your gadgets or to email given by you.
Step 4: Make duplicates of your template. This can save you from potential difficulties. We cannot see or disclose your details, therefore you can relax knowing it is protected.
