
Should you want to fill out how to cms oxygen, you don't have to install any kind of programs - just give a try to our PDF tool. Our tool is consistently evolving to provide the very best user experience attainable, and that's due to our commitment to constant enhancement and listening closely to comments from customers. With some easy steps, you are able to begin your PDF journey:
Step 1: First, access the pdf editor by clicking the "Get Form Button" above on this site.
Step 2: This tool offers the ability to customize your PDF in various ways. Change it with personalized text, adjust what is originally in the document, and put in a signature - all when you need it!
Concentrate while completing this document. Make sure every blank field is filled in properly.
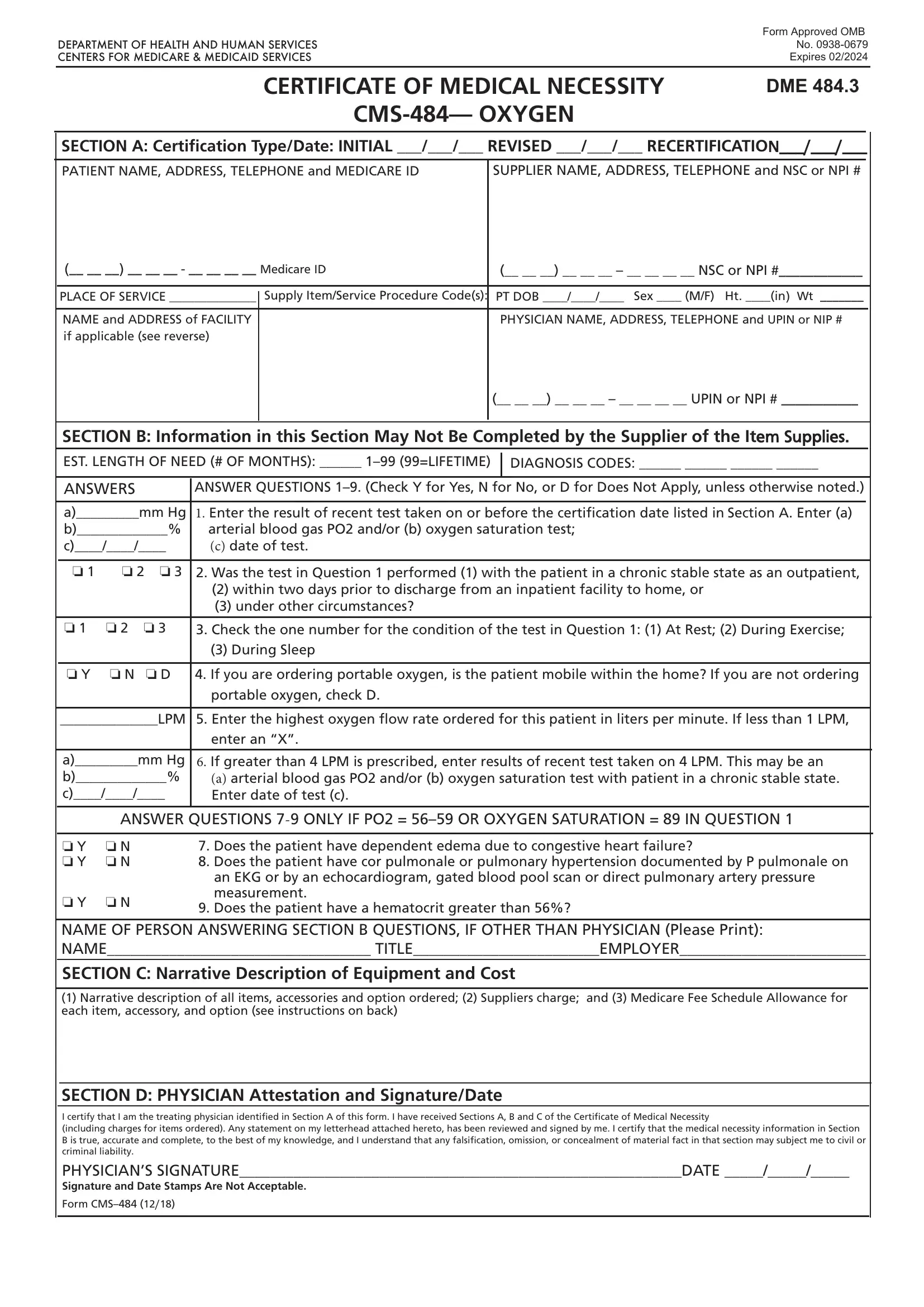
1. The how to cms oxygen necessitates specific information to be typed in. Be sure that the subsequent blanks are finalized:
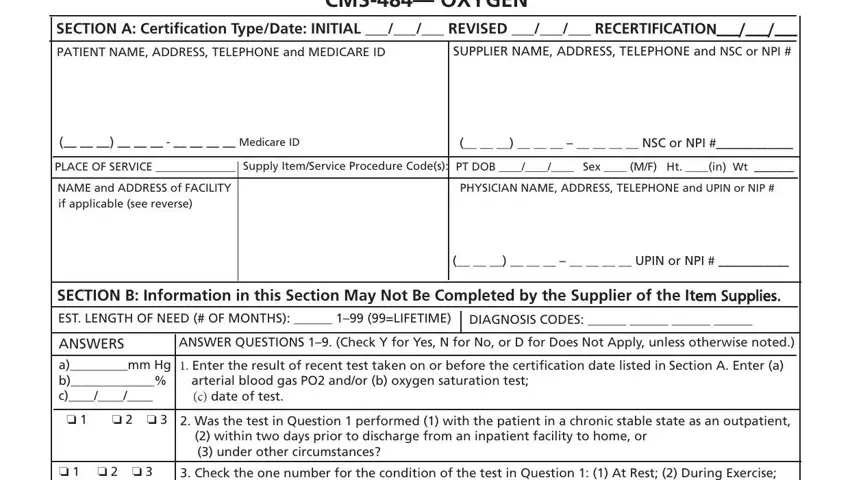
2. Right after filling out this part, go on to the subsequent step and fill in the essential particulars in all these blank fields - o o o, o Y o N o D, During Sleep, If you are ordering portable, portable oxygen check D, LPM Enter the highest oxygen flow, enter an X, amm Hg b c, If greater than LPM is, a arterial blood gas PO andor b, ANSWER QUESTIONS ONLY IF PO OR, o Y o N o Y o N, Does the patient have dependent, o N, and an EKG or by an echocardiogram.
3. This next step is straightforward - complete all the empty fields in SECTION D PHYSICIAN Attestation to complete the current step.

Always be extremely careful while filling in SECTION D PHYSICIAN Attestation and SECTION D PHYSICIAN Attestation, as this is the section in which a lot of people make errors.
Step 3: Just after going through your form fields, click "Done" and you are done and dusted! Grab your how to cms oxygen when you sign up for a free trial. Easily gain access to the pdf form inside your FormsPal account page, with any edits and changes automatically kept! At FormsPal, we do everything we can to be sure that your information is stored secure.