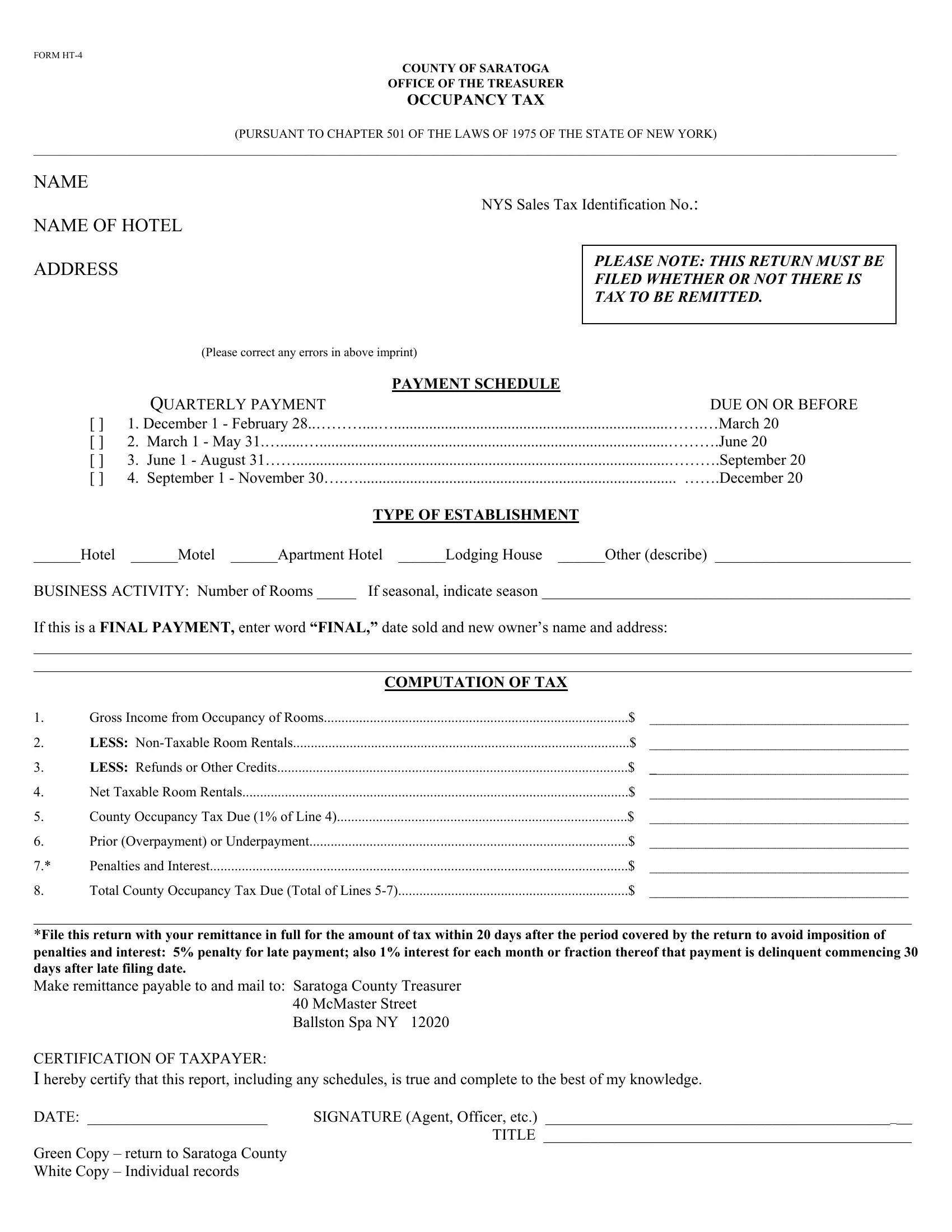
In the scenic County of Saratoga, nestled within the vibrant state of New York, hotel and lodging establishments are familiar with a crucial document known as Form HT-4. This form plays an integral role in the financial operations of such businesses, as it is a key component in the administration of the occupancy tax, mandated by Chapter 501 of the Laws of 1975 of the State of New York. The details stipulated on the form include identifying information about the establishment, such as the name of the hotel and the address, alongside the New York State Sales Tax Identification Number. Importantly, it underscores the requirement for entities to file this return within specific deadlines—regardless of whether there is tax to be remitted or not—thus ensuring compliance with local tax legislation. The form meticulously lays out the payment schedule, dividing the year into quarters, each with its own deadline for submission. Furthermore, it requires establishments to categorize their business activity and declare the number of rooms they operate, providing options for those operating seasonally. It is also designed to capture changes in ownership and final payments. The computation section of the form is designed to quantify the taxable income derived from room occupancies, after accounting for non-taxable rentals and any refunds or credits, culminating in the calculation of the occupancy tax due. Penalties for late submissions are clearly delineated, emphasizing the importance of adherence to the deadlines. By affording a comprehensive overview of the occupancy tax process, Form HT-4 serves as a critical tool for ensuring that hotels, motels, and other lodging facilities contribute fair and accurate tax amounts to the local treasury, reinforcing the financial infrastructure of Saratoga County.
| Question | Answer |
|---|---|
| Form Name | Form Ht 4 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | saratoga form download, saratoga form print, form ht 4, saratoga form online |

FORM
COUNTY OF SARATOGA
OFFICE OF THE TREASURER
OCCUPANCY TAX
(PURSUANT TO CHAPTER 501 OF THE LAWS OF 1975 OF THE STATE OF NEW YORK)
__________________________________________________________________________________________________________________________________________
NAME
NAME OF HOTEL
ADDRESS
NYS Sales Tax Identification No.:
PLEASE NOTE: THIS RETURN MUST BE
FILED WHETHER OR NOT THERE IS
TAX TO BE REMITTED.
(Please correct any errors in above imprint)
|
PAYMENT SCHEDULE |
QUARTERLY PAYMENT |
DUE ON OR BEFORE |
[] 1. December 1 - February 28..………....…......................................................................…….…March 20
[] 2. March 1 - May 31.…......….........................................................................................……….June 20
[] 3. June 1 - August 31……...............................................................................................……….September 20
[] 4. September 1 - November 30….…................................................................................. …….December 20
TYPE OF ESTABLISHMENT
______Hotel ______Motel ______Apartment Hotel ______Lodging House ______Other (describe) _________________________
BUSINESS ACTIVITY: Number of Rooms _____ If seasonal, indicate season _______________________________________________
If this is a FINAL PAYMENT, enter word “FINAL,” date sold and new owner’s name and address:
________________________________________________________________________________________________________________
________________________________________________________________________________________________________________
|
COMPUTATION OF TAX |
|
|
1. |
Gross Income from Occupancy of Rooms |
$ |
_____________________________________ |
2. |
LESS: |
$ |
_____________________________________ |
3. |
LESS: Refunds or Other Credits |
$ |
_____________________________________ |
4. |
Net Taxable Room Rentals |
$ |
_____________________________________ |
5. |
County Occupancy Tax Due (1% of Line 4) |
$ |
_____________________________________ |
6. |
Prior (Overpayment) or Underpayment |
$ |
_____________________________________ |
7.* |
Penalties and Interest |
$ |
_____________________________________ |
8. |
Total County Occupancy Tax Due (Total of Lines |
$ |
_____________________________________ |
________________________________________________________________________________________________________________
*File this return with your remittance in full for the amount of tax within 20 days after the period covered by the return to avoid imposition of penalties and interest: 5% penalty for late payment; also 1% interest for each month or fraction thereof that payment is delinquent commencing 30 days after late filing date.
Make remittance payable to and mail to: Saratoga County Treasurer 40 McMaster Street Ballston Spa NY 12020
CERTIFICATION OF TAXPAYER:
I hereby certify that this report, including any schedules, is true and complete to the best of my knowledge.
DATE: _______________________ |
SIGNATURE (Agent, Officer, etc.) _______________________________________________ |
|
TITLE _______________________________________________ |
Green Copy – return to Saratoga County |
|
White Copy – Individual records |
|