As a business owner, you will likely have to file form LS 355 with the Illinois Department of Revenue. This form is used to report certain information about your company, including its total revenue and taxable income. Knowing what this form entails and how to complete it correctly is important for ensuring that your business is in compliance with state tax laws. In this article, we will provide an overview of what form LS 355 is and how to fill it out correctly. We will also discuss some of the penalties that may be imposed for incorrect or late filings. So if you are wondering whether or not you need to file form LS 355, or if you are unsure how to complete it, keep reading!
| Question | Answer |
|---|---|
| Form Name | Form Ls 355 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | DB-100, FEIN, LS-355, DB-155 |
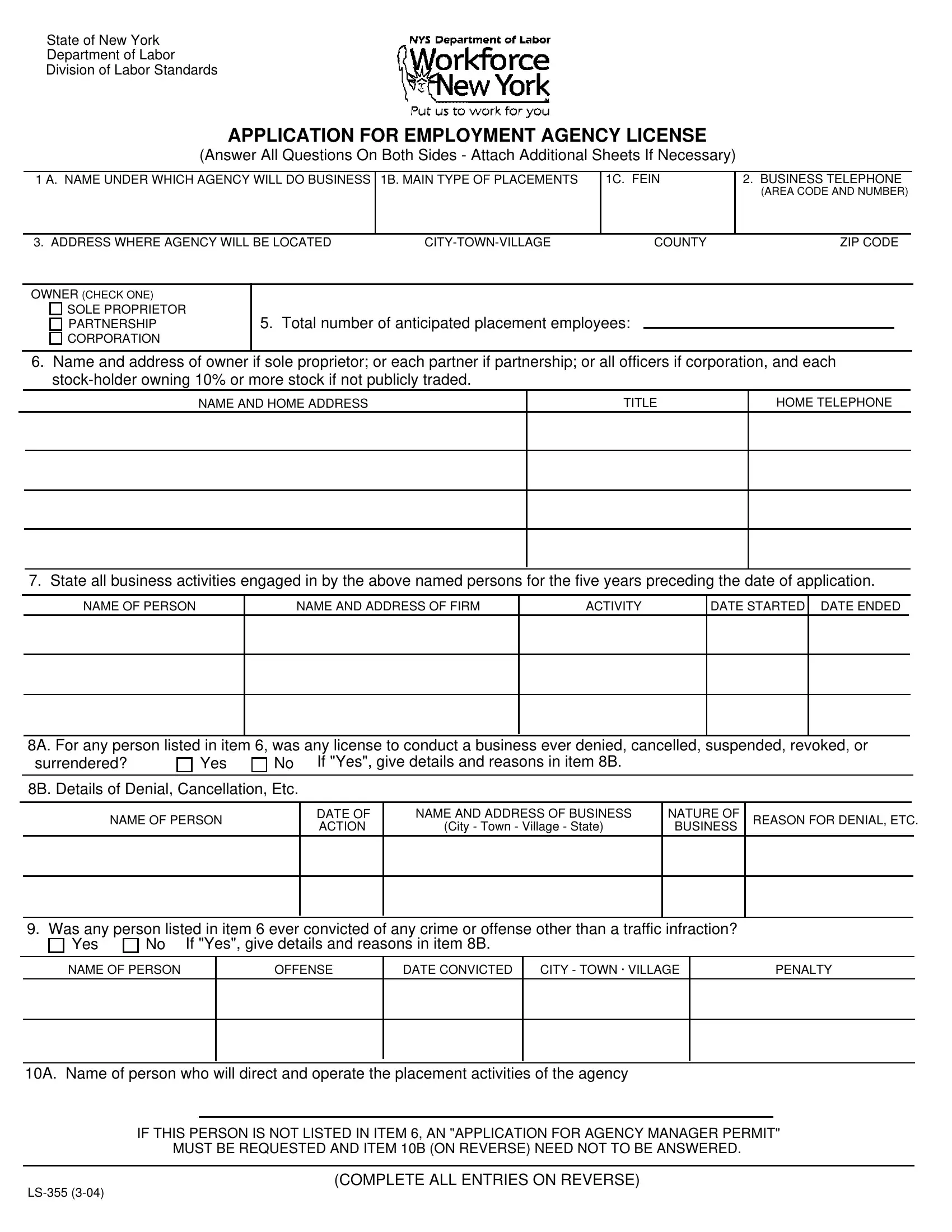
State of New York
Department of Labor
Division of Labor Standards
APPLICATION FOR EMPLOYMENT AGENCY LICENSE
(Answer All Questions On Both Sides - Attach Additional Sheets If Necessary)
1 A. NAME UNDER WHICH AGENCY WILL DO BUSINESS
1B. MAIN TYPE OF PLACEMENTS
1C. FEIN
2.BUSINESS TELEPHONE
(AREA CODE AND NUMBER)
3. ADDRESS WHERE AGENCY WILL BE LOCATED |
COUNTY |
ZIP CODE |
OWNER (CHECK ONE)
SOLE PROPRIETOR PARTNERSHIP CORPORATION
5. Total number of anticipated placement employees:
6.Name and address of owner if sole proprietor; or each partner if partnership; or all officers if corporation, and each
NAME AND HOME ADDRESS
TITLE
HOME TELEPHONE
7. State all business activities engaged in by the above named persons for the five years preceding the date of application.
NAME OF PERSON
NAME AND ADDRESS OF FIRM
ACTIVITY
DATE STARTED DATE ENDED
8A. For any person listed in item 6, was any license to conduct a business ever denied, cancelled, suspended, revoked, or
surrendered?
Yes
No If "Yes", give details and reasons in item 8B.
8B. Details of Denial, Cancellation, Etc.
NAME OF PERSON
DATE OF ACTION
NAME AND ADDRESS OF BUSINESS
(City - Town - Village - State)
NATURE OF BUSINESS
REASON FOR DENIAL, ETC.
9. Was any person listed in item 6 ever convicted of any crime or offense other than a traffic infraction?
Yes |
No If "Yes", give details and reasons in item 8B. |
NAME OF PERSON
OFFENSE
DATE CONVICTED
CITY - TOWN · VILLAGE
PENALTY
10A. Name of person who will direct and operate the placement activities of the agency
IF THIS PERSON IS NOT LISTED IN ITEM 6, AN "APPLICATION FOR AGENCY MANAGER PERMIT" MUST BE REQUESTED AND ITEM 10B (ON REVERSE) NEED NOT TO BE ANSWERED.
(COMPLETE ALL ENTRIES ON REVERSE)
10B. List each employer for whom person listed in item 10A worked as a placement employee, vocational counselor, or
in related activities. Include
NAME AND ADDRESS
DATE
STARTED
DATE ENDED
DUTIES (give detailed listing, showing percent of time spent at interviewing and counseling applicants; screening, selecting and placing applicants; soliciting and obtaining job orders; preparing job descriptions, etc. and time spent on
11. Does applicant intend to recruit persons from outside the State for employment as domestic or household employees?
Yes |
No If "Yes", give details regarding each emigrant agent. Submit photostatic copy of each licensed agent's license. |
NAME AND ADDRESS
OF
EMIGRANT AGENT
STATE
(Country If not U S )
IN WHICH OPERATING
LICENSE NUMBER
DATE
LICENSE EXPIRES
NAME, ADDRESS, TITLE
OF ISSUING OFFICIAL
12. Does applicant intend to provide or arrange for lodging for applicants for employment or for person doing business
with the agency? |
Yes |
No If "Yes", give details regarding each location. |
NAME AND ADDRESS Of PREMISES WHERE LODGING WILL BE FURNISHED
TELEPHONE
NUMBER
NAME OF PERSON
IN CHARGE
13. Does applicant provide hospitalization insurance for overseas domestics? |
Yes |
No If "Yes", give name |
of insurance company and policy number. |
|
|
NAME OF INSURANCE COMPANY
POLICY NUMBER
NOTE
Application must be accompanied by: (a) surety bond naming the people of the State of New York as obligee, in the penal sum of $5,000, except penal sum of $10,000 required for modeling agencies and agencies engaged in recruiting domestic or household employees from outside the continental United States; (b) completed fingerprint card(s) for each person listed in item #6 of this application; (c) two statements of character for each person listed in item #6 of this application; (d) check or money order for the required fee, payable to the Commissioner of Labor; (e) separate U.S. $75.00 certified check or postal money order only for the required fingerprint search and verification ($75.00 for each search), payable to the New York State Division of Criminal Justice Services (Note: No personal checks will be accepted); (f) two samples of each form that applicants will be required to sign (g) photocopies of each licensed emigrant agent's license; (h) if sole owner or partnership, certified copy of certificate of doing business as filed with the county clerk. If corporation, photocopy of corporate filing receipt as filed with Secretary of State; (i) FROM YOUR INSURANCE COMPANY, you must obtain a completed
If NOT liable for WC and/or disability insurance, provide completed
IMPORTANT PROMPT NOTIFICATION REQUIRED OF ANY CHANGE OF AGENCY NAME, ADDRESS, MANAGER OWNERSHIP, PARTNERS, OFFICERS OR STOCKHOLDERS. PRIOR APPROVAL WILL BE REQUIRED.
THE STATEMENTS MADE IN THIS APPLICATION ARE SUBSCRIBED AND AFFIRMED BY ME AS TRUE UNDER THE PENALTIES OF PERJURY.
14. Signature of owner. If a corporation, must be signed by president and treasurer; if a partnership, by all partners.
SIGNATURE(S) OF PERSON(S) MAKING APPLICATIONS
TITLE
DATE
ALL INFORMATION AND MATERIAL SUBMITTED IS SUBJECT TO INVESTIGATION BY THIS DEPARTMENT