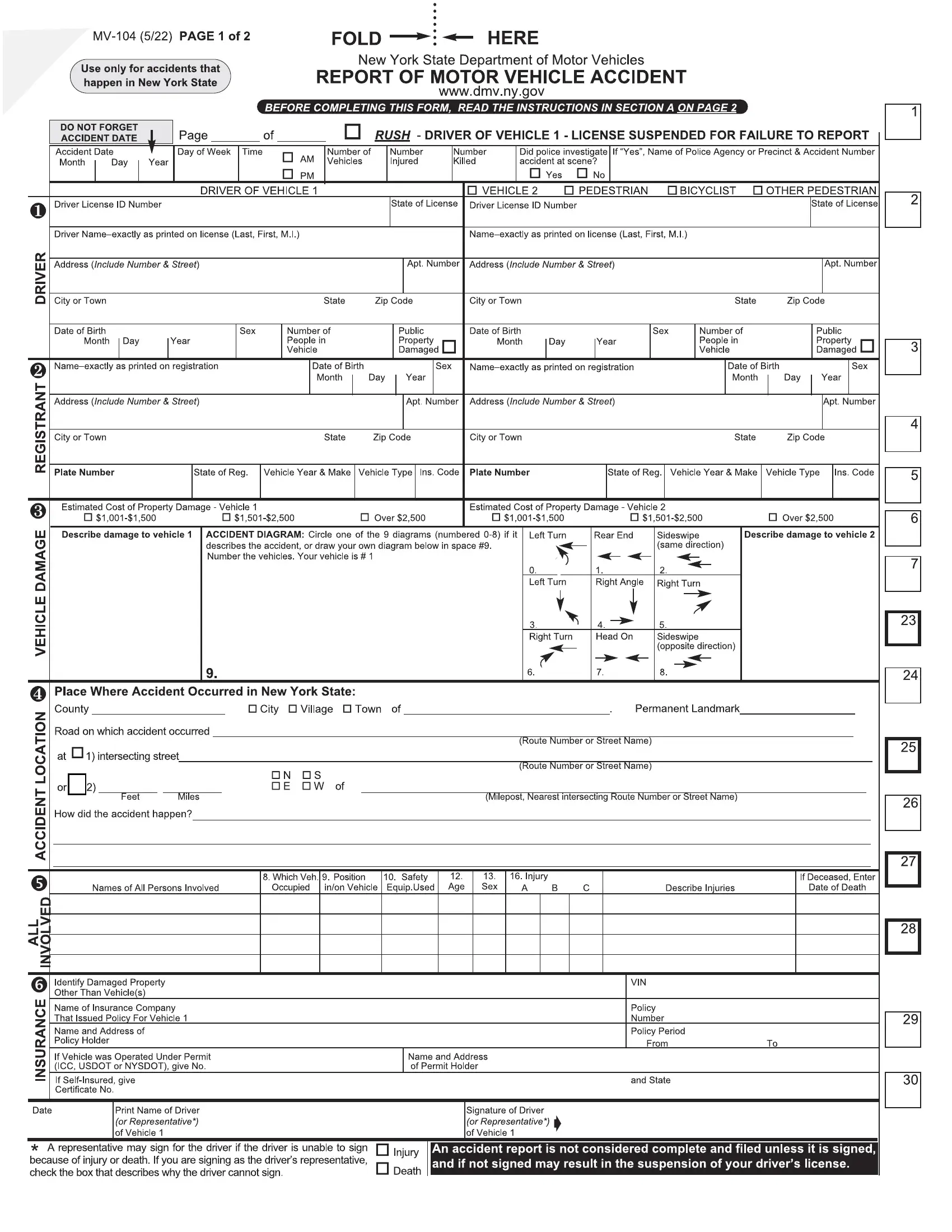

The MV-104 form reports motor vehicle accidents to the New York State DMV. Completing this form accurately is very important for legal and insurance purposes. Below is a step-by-step guide on how to fill it out.
1. Gather Information
Before filling out the form, collect all necessary information regarding the accident. This covers the date, time, and location of the accident, as well as details about the vehicles, drivers, and any injuries sustained.
2. Fill Out Accident Information
Write the exact date and time of the accident. Specify the location with as much detail as possible, including the street name, the nearest cross street, and the city or town.
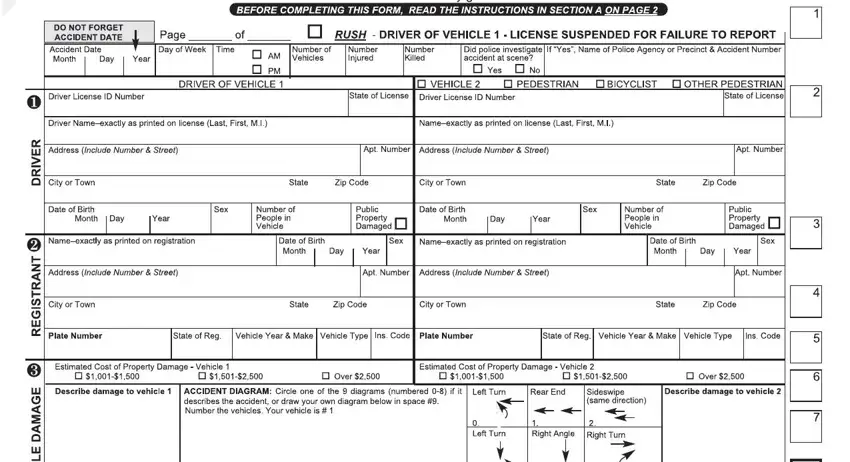
3. Vehicle Information
Provide detailed information for each vehicle involved in the accident. This includes the make, model, year, and license plate number. Additionally, indicate the extent of damage to each vehicle.
4. Driver Information
For each vehicle involved, fill in the driver’s information, including name, address, driver's license number, and insurance details. Ensure this information is accurate to avoid issues with insurance claims.
5. Diagram of the Accident
Draw a diagram of the accident scene in the space provided. Include the position of each vehicle before and after the collision, and mark the direction each was traveling.
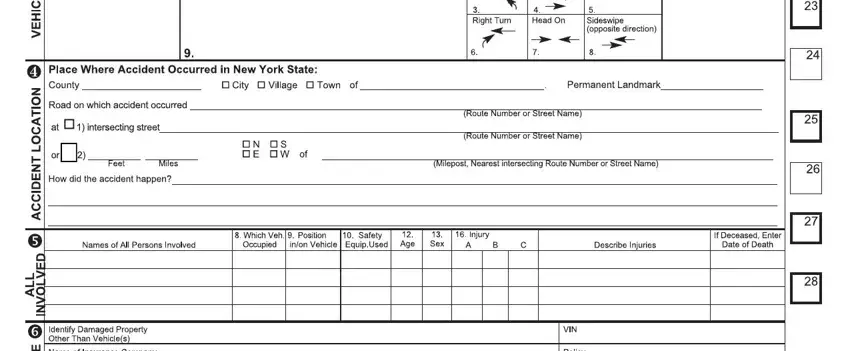
6. Description of the Accident
In the narrative section, describe the accident in detail. Include any relevant information that the diagram does not show, such as weather conditions, road quality, or any obstacles that played a role in the accident.
7. Witness Information
If there were any witnesses to the accident, provide their names and contact information. Witness accounts can be crucial in determining fault in complex accident scenarios.
8. Review and Sign
Review the information for accuracy. Once you know all the complete details, sign and date the form. Your signature verifies that the information is accurate to the best of your knowledge.
9. Submit the Form
Finally, submit the completed form to the DMV. Be sure to keep a copy for your records and insurance purposes.