We used the top-rated software engineers to set-up our PDF editor. The app will help you fill in the Form Owcp 5C form conveniently and won't consume a great deal of your time. This simple guide can help you begin.
Step 1: Hit the orange "Get Form Now" button on this web page.
Step 2: You will discover all of the options that you may take on the document once you have accessed the Form Owcp 5C editing page.
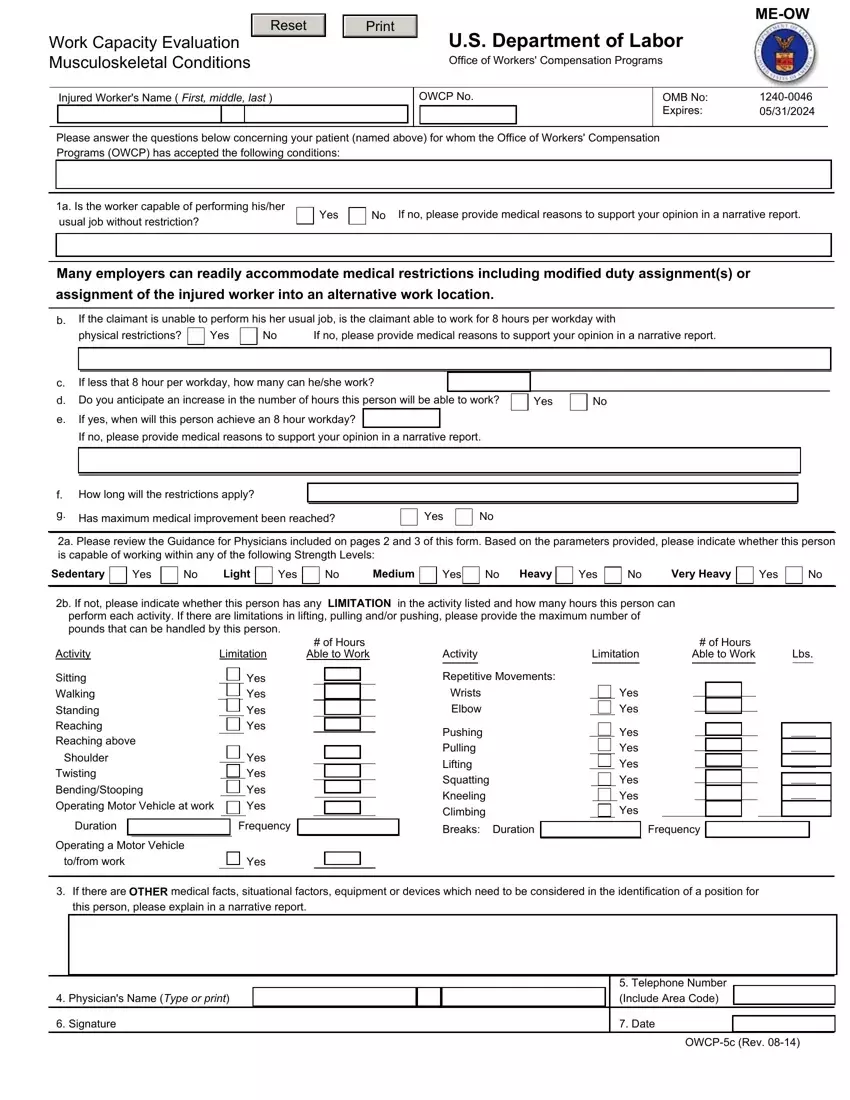
Complete the Form Owcp 5C PDF by providing the information meant for each individual area.
Fill out the If no please provide medical, How long will the restrictions, Has maximum medical improvement, Yes, a Please review the Guidance for, Sedentary, Yes, Light, Yes, Medium, Yes, Heavy, Yes, Very Heavy, and Yes areas with any particulars that may be asked by the program.
You should be requested for some necessary data so you can fill up the Twisting BendingStooping Operating, Yes Yes Yes Yes, Duration, Frequency, Operating a Motor Vehicle, tofrom work, Yes, Pushing Pulling Lifting Squatting, Yes Yes Yes Yes Yes Yes, Breaks, Duration, Frequency, If there are OTHER medical facts, Physicians Name Type or print, and Signature area.
Step 3: Choose the Done button to make certain that your finalized document can be transferred to each electronic device you decide on or delivered to an email you specify.
Step 4: Generate copies of your document. This is going to save you from upcoming concerns. We cannot see or share the information you have, thus you can relax knowing it will be safe.
