The PDF editor was made with the intention of making it as effortless and easy-to-use as possible. These steps can certainly make completing the owcp dol forms fast and simple.
Step 1: Click on the "Get Form Here" button.
Step 2: At the moment you're on the document editing page. You may change and add information to the form, highlight words and phrases, cross or check certain words, include images, put a signature on it, get rid of unneeded areas, or take them out entirely.
To fill out the file, enter the details the platform will request you to for each of the following areas:
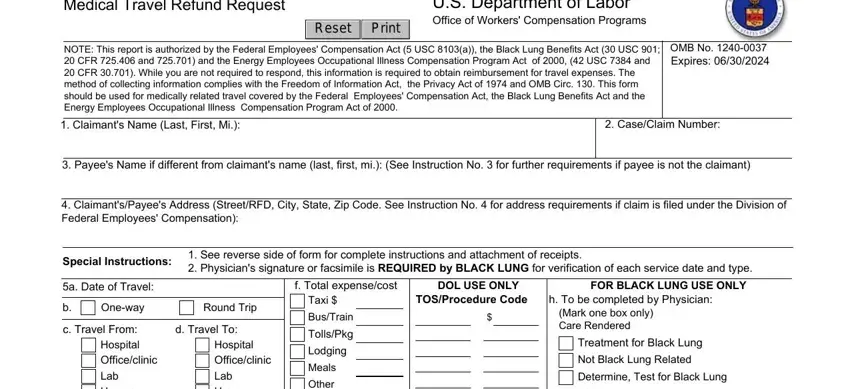
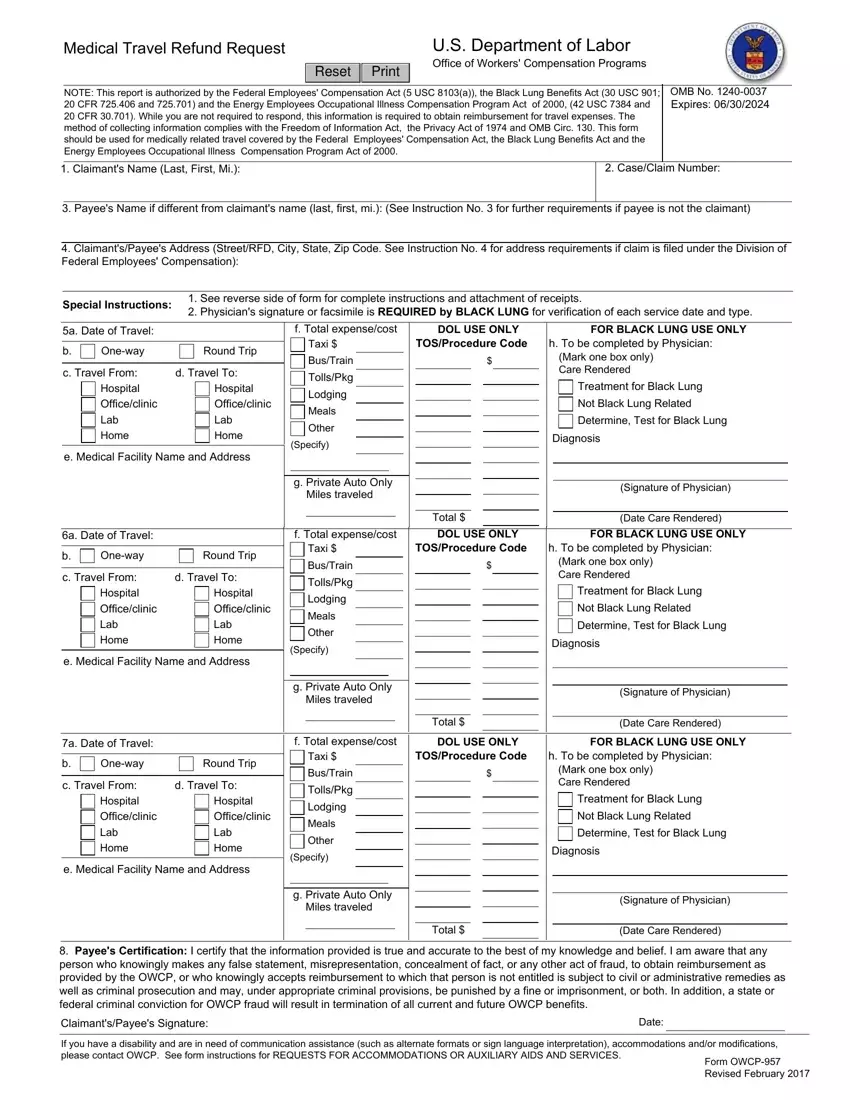
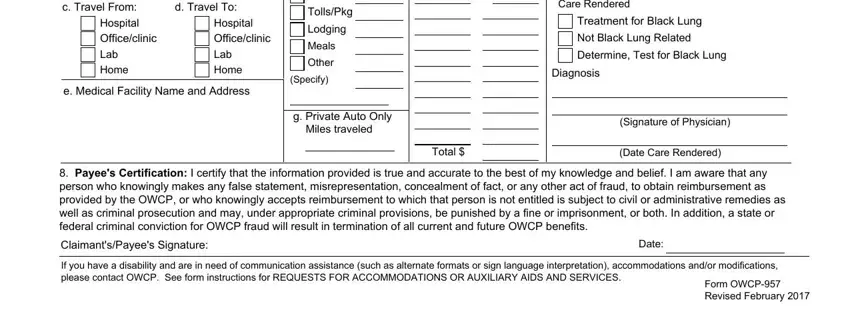
Enter the demanded particulars in the area c Travel From Hospital, Hospital Officeclinic Lab Home, e Medical Facility Name and Address, Other, Specify, Diagnosis, g Private Auto Only Miles traveled, Signature of Physician, Total, Date Care Rendered, a Date of Travel, f Total expensecost, DOL USE ONLY, FOR BLACK LUNG USE ONLY, and Oneway.
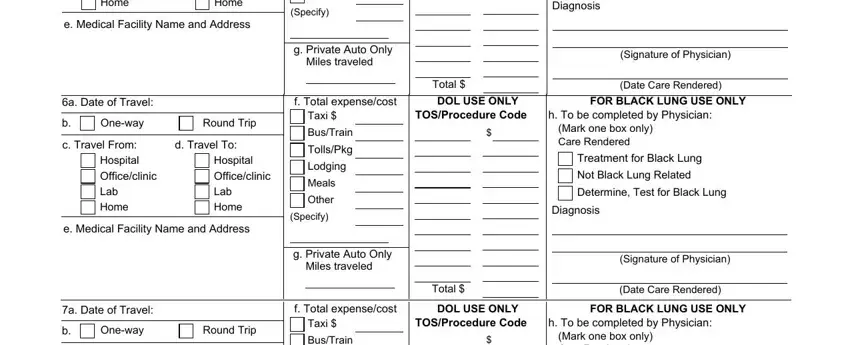
In the c Travel From Hospital, d Travel To, Hospital Officeclinic Lab Home, e Medical Facility Name and Address, BusTrain, TollsPkg, Lodging, Meals, Other, Specify, Mark one box only Care Rendered, Treatment for Black Lung, Not Black Lung Related, Determine Test for Black Lung, and Diagnosis area, emphasize the valuable details.
Take the time to list the rights and obligations of the sides in the Please explain the following, a Relationship to the claimant, b The reason you are requesting, Enter the address of the person, Note If your claim is filed under, For the FECA program to effectuate, and Complete a separate block, a Enter date of travel, b Mark one box only, c Mark one box only, d Mark one box only, and e Enter the name and address of space.
Step 3: When you press the Done button, your ready document can be simply transferred to any of your gadgets or to electronic mail stated by you.
Step 4: Create duplicates of the form - it will help you stay away from potential future concerns. And don't worry - we do not publish or view the information you have.
