
In case you wish to fill out opioid, you don't have to download any kind of applications - simply make use of our PDF editor. In order to make our editor better and more convenient to utilize, we consistently develop new features, with our users' suggestions in mind. All it takes is a couple of simple steps:
Step 1: First, access the pdf editor by clicking the "Get Form Button" in the top section of this site.
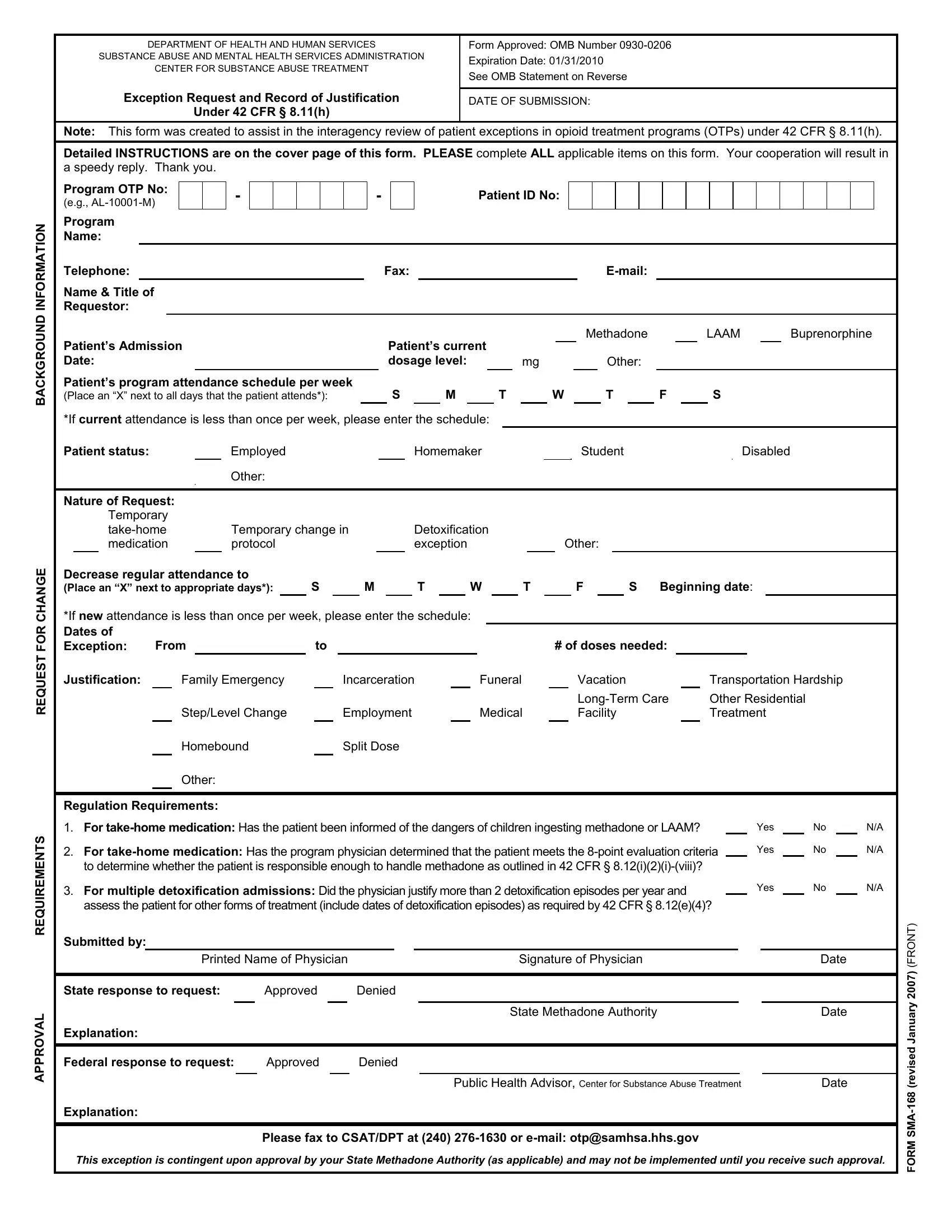
Step 2: As soon as you access the online editor, there'll be the document ready to be filled out. Aside from filling out different fields, you could also do other things with the PDF, including writing any textual content, editing the original textual content, adding images, placing your signature to the form, and a lot more.
As for the blank fields of this particular form, here is what you should know:
1. While filling out the opioid, make certain to incorporate all needed fields in its relevant area. It will help to facilitate the process, allowing for your details to be handled efficiently and appropriately.
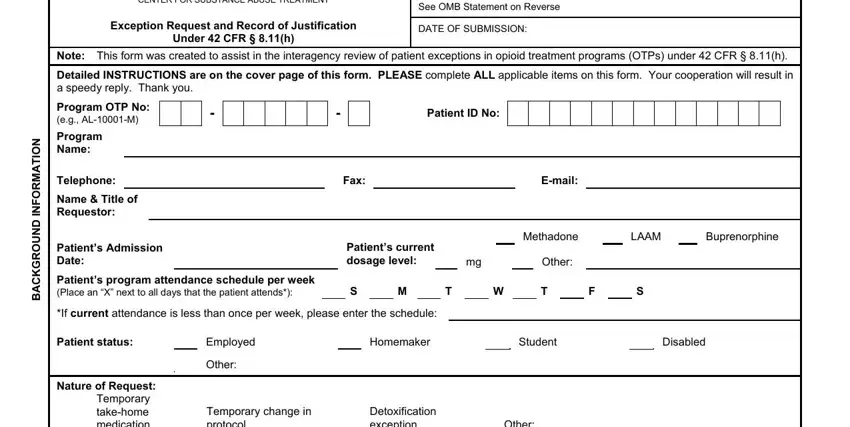
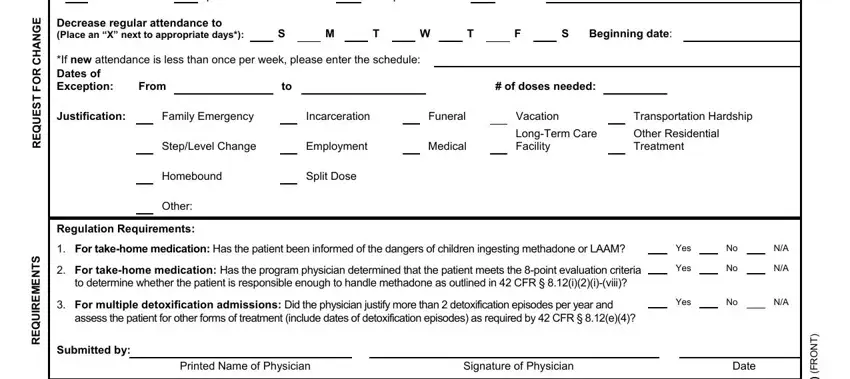
2. Soon after filling in this step, head on to the next stage and fill in all required details in all these blank fields - Temporary takehome medication, Temporary change in protocol, Detoxification exception, Other, Decrease regular attendance to, If new attendance is less than, From, Beginning date, of doses needed, Justification, Family Emergency, StepLevel Change, Homebound, Incarceration, and Employment.
People generally make some mistakes while filling in Temporary takehome medication in this section. You should re-examine whatever you type in here.
3. This third stage is hassle-free - fill out all of the fields in L A V O R P P A, Date, T N O R F y r a u n a J d e, v e r A M S M R O F, State response to request, Approved, Denied, Explanation, Federal response to request, Approved, Denied, Explanation, State Methadone Authority, Public Health Advisor Center for, and Date to finish this part.
Step 3: Once you've looked over the details in the fields, simply click "Done" to finalize your FormsPal process. Try a 7-day free trial subscription with us and gain immediate access to opioid - downloadable, emailable, and editable in your personal account. FormsPal provides secure document tools with no data record-keeping or distributing. Be assured that your information is safe here!