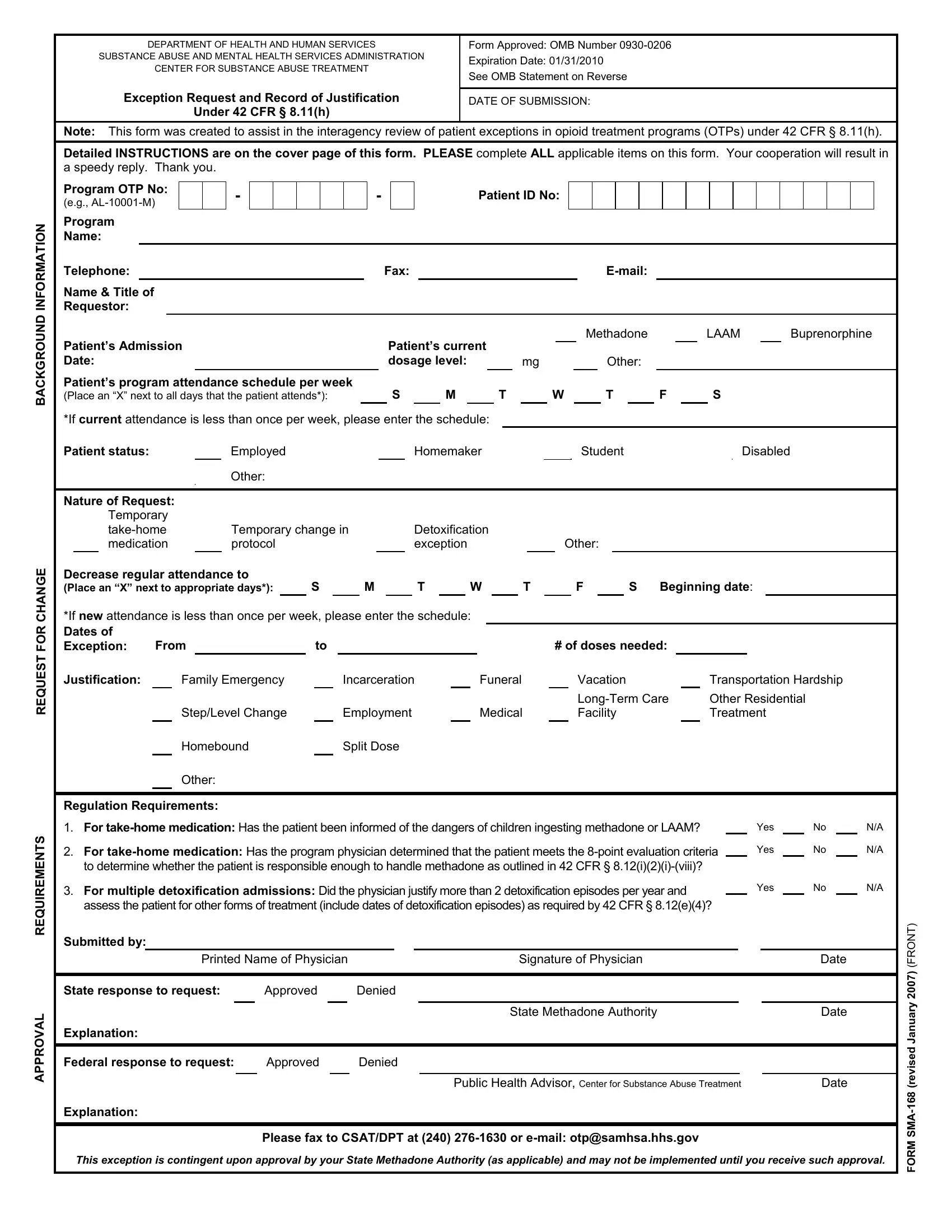
In the intricate landscape of healthcare administration, forms and documentation serve as the backbone for ensuring compliance, facilitating communication, and enhancing the quality of care. Among these, the SMA-168 form stands out as a particularly important document within the domain of opioid treatment programs (OTPs). Developed by the Substance Abuse and Mental Health Services Administration (SAMHSA), a branch of the Department of Health and Human Services, this form plays a crucial role in documenting exceptions for patients in opioid treatment settings. Designed under the regulatory framework of 42 CFR § 8.11(h), the SMA-168 form assists in the interagency review process by providing a structured format for submitting and justifying requests for exceptions to standard treatment protocols. Such exceptions could include requests for take-home medications, modifications in treatment protocols, or exemptions due to specific personal circumstances such as employment, medical issues, or family emergencies. Beyond its immediate administrative function, the form underscores the commitment of healthcare regulators and providers to accommodate the varying needs of individuals undergoing opioid treatment, balancing regulatory compliance with flexibility. The form not only details the specific nature of each request but also includes evaluation criteria for take-home medications and the requirement for a physician’s justification in certain scenarios. This process ensures each request is considered thoughtfully, acknowledging the individual's situation while maintaining the integrity and safety of the treatment program.
| Question | Answer |
|---|---|
| Form Name | Form Sma 168 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | otpsamhsa, 8-point, E-mail, Requestor |