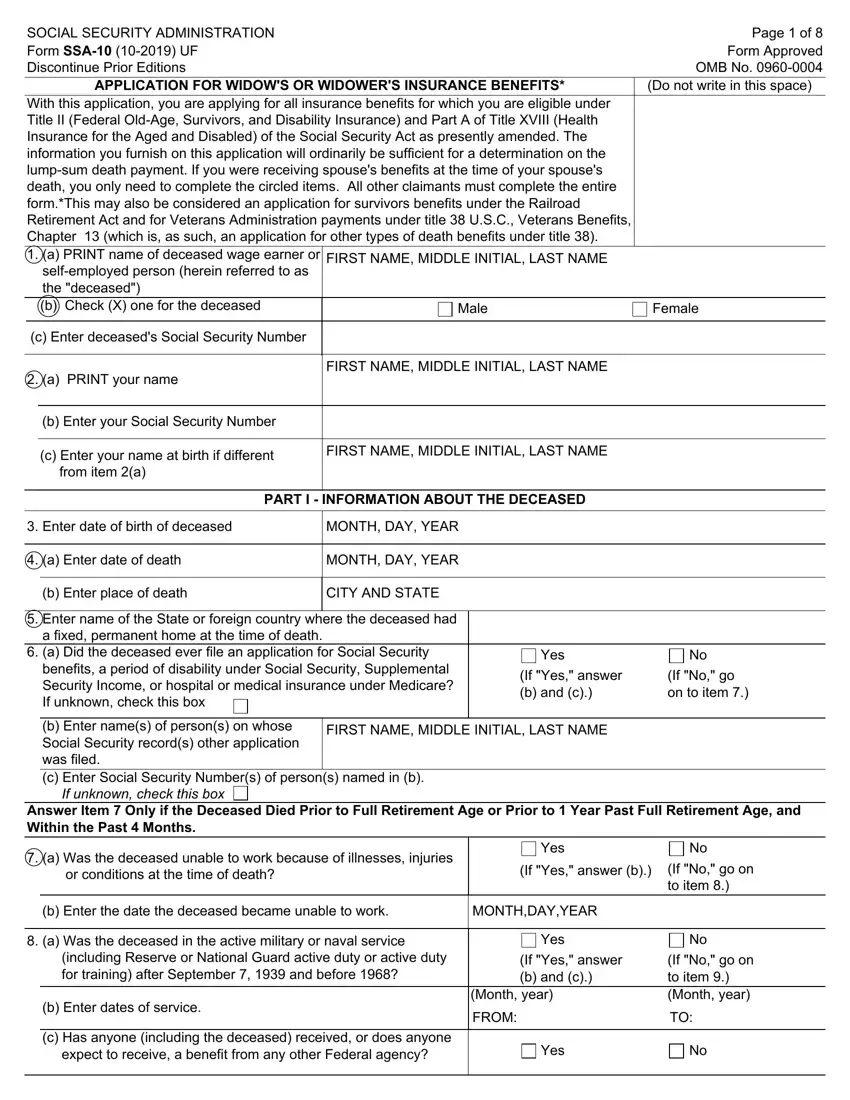
Navigating the Social Security Administration's Form SSA-10, an essential document for individuals applying for widow's or widower's insurance benefits, reveals the comprehensive nature of this application process. This form serves not only as an application for insurance benefits under Title II, which encompasses Federal Old-Age, Survivors, and Disability Insurance, but also under Part A of Title XVIII for Health Insurance for the Aged and Disabled. Its detailed structure is designed to capture sufficient information for determining eligibility for a lump-sum death payment and potentially other benefits including those under the Railroad Retirement Act and Veterans Administration payments. Applicants find sections dedicated to providing information about the deceased, including their Social Security contribution history and military service, as well as pertinent details about the applicant's relationship to the deceased, their own work history, and marital background. Importantly, the form also addresses the possibility of receiving Medicare benefits, highlighting the interconnection between various government benefits following the loss of a spouse. Completion of this form requires thorough attention to detail, as it directly impacts the applicant's eligibility for benefits and the financial support they can receive during a challenging period of adjustment.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 10 |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | ssa 10, social security ssa 10 form, form ssa 1099 social security statement, social security administration form ssa 10 |
