Managing forms with our PDF editor is simpler in comparison with anything. To modify ssa 623 the file, there is nothing for you to do - basically keep to the steps below:
Step 1: The first step should be to choose the orange "Get Form Now" button.
Step 2: Now, you're on the form editing page. You may add information, edit present data, highlight specific words or phrases, put crosses or checks, insert images, sign the document, erase unrequired fields, etc.
The PDF document you plan to fill in will consist of the following segments:
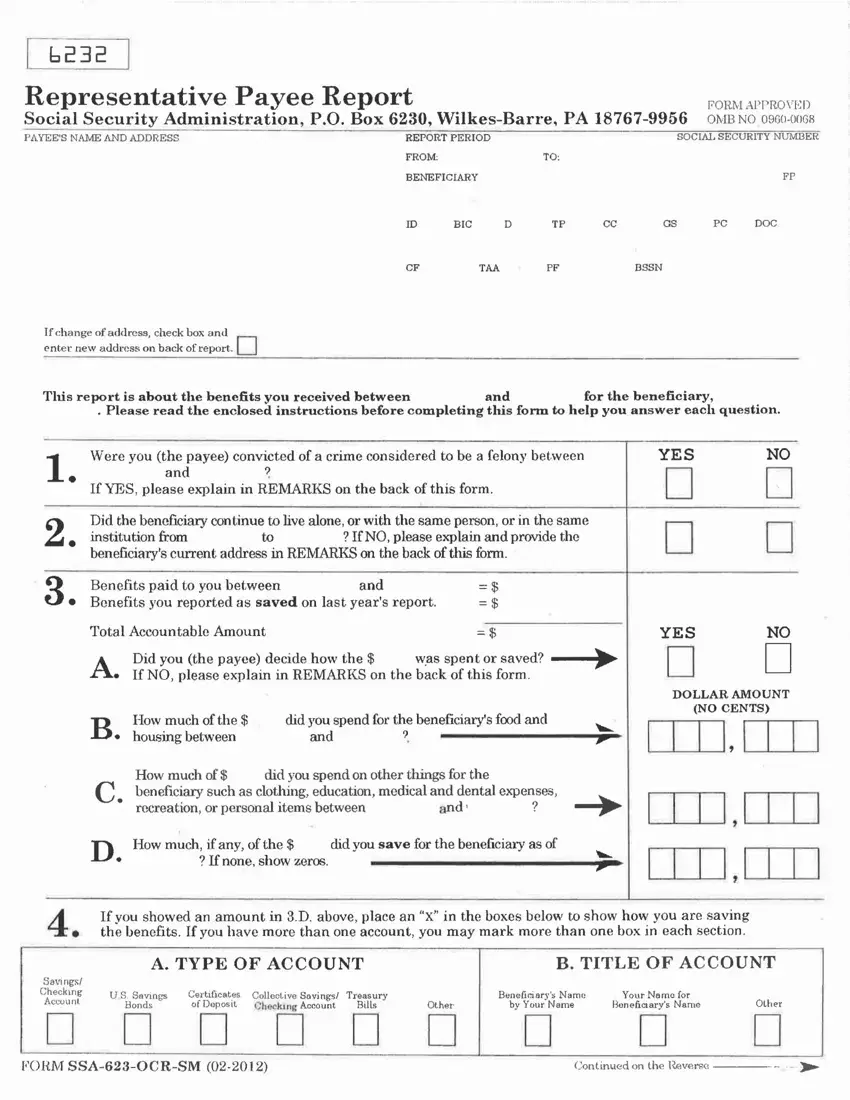
In the section If, NO, please, explain, and, provide, the and, Total, Accountable, Amount housing, between and, and, DHow, much, if, any, of, the If, none, show, zeros did, you, save, for, the, beneficiary, as, of YES, DOLLAR, AMOUNT and NO, CENTS enter the data that the application requests you to do.
Within the field talking about Savings, Checking, Account US, Savings Bonds, Certificates, of, Deposit CollectiveSavings, Checking, Account Treasury, Bills, Other, Beneficiary, s, Name b, v, Your, Name Your, Name, for Bone, fi, ciar, vs, Name Other, FORMS, SAO, CRS, M and Continued, on, the, Inverse make sure you type in some essential data.

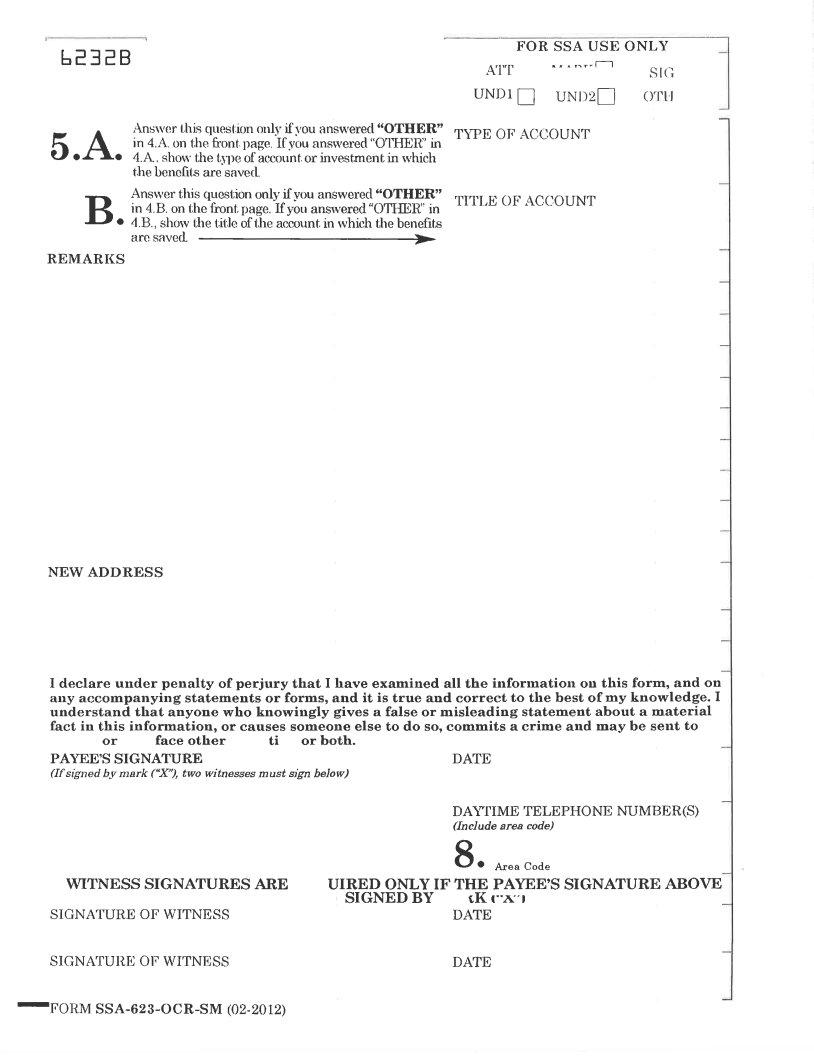
Explain the rights and obligations of the sides in the box are, saved TYPE, OF, ACCOUNT TITLE, OF, ACCOUNT and REMARKS.
Finalize by checking the next areas and submitting the relevant data: NEW, ADDRESS and DATE, g, Area, Code
Step 3: As soon as you click the Done button, the completed file is readily transferable to all of your gadgets. Alternatively, you may send it using mail.
Step 4: To stay away from potential forthcoming risks, you need to hold a minimum of two or more copies of any file.
