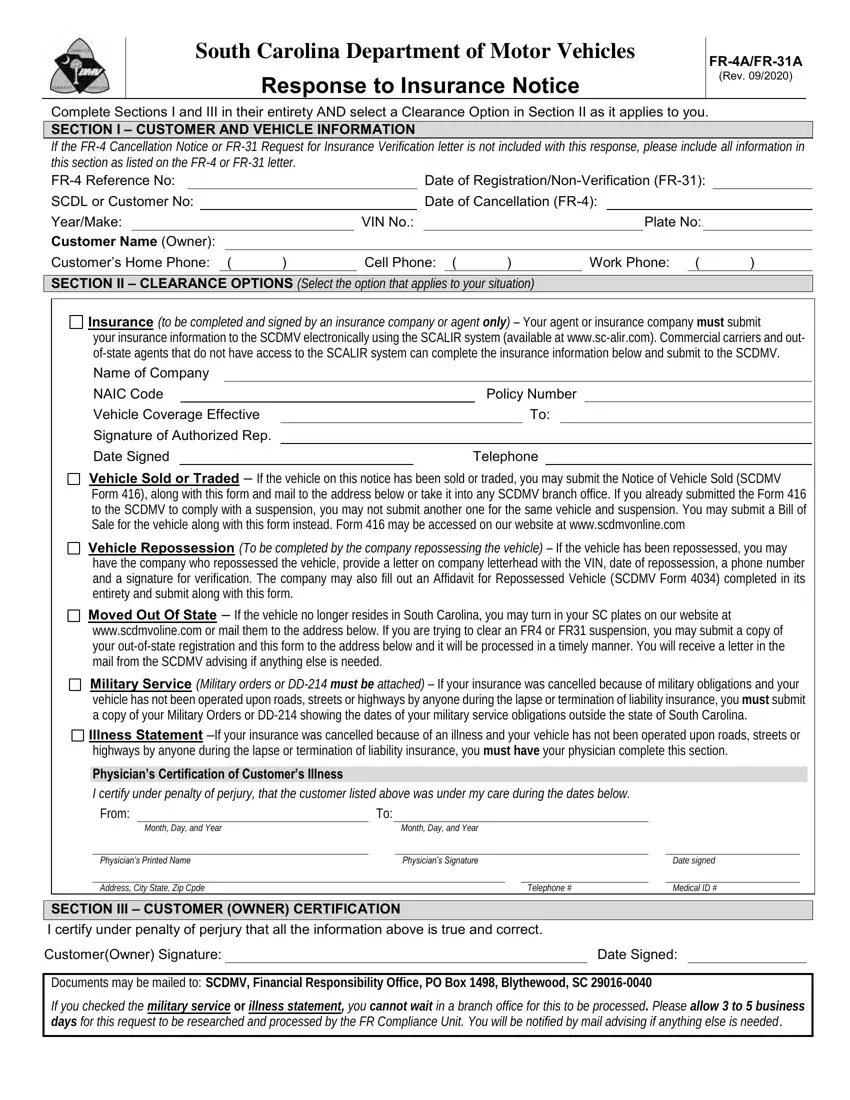
Complete Sections I and III in their entirety AND select a Clearance Option in Section II as it applies to you.
SECTION I – CUSTOMER AND VEHICLE INFORMATION
If the FR-4 Cancellation Notice or FR-31 Request for Insurance Verification letter is not included with this response, please include all information in this section as listed on the FR-4 or FR-31 letter.
FR-4 Reference No: |
|
|
|
|
Date of Registration/Non-Verification (FR-31): |
|
SCDL or Customer No: |
|
|
|
|
Date of Cancellation (FR-4): |
|
|
|
|
Year/Make: |
|
|
VIN No.: |
|
|
|
|
Plate No:. |
|
|
Customer Name (Owner): |
|
|
|
|
|
|
|
|
|
|
|
|
|
Customer’s Home Phone: ( |
) |
Cell Phone: ( |
) |
Work Phone: |
( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION II – CLEARANCE OPTIONS (Select the option that applies to your situation)
Insurance (to be completed and signed by an insurance company or agent only) – Your agent or insurance company must submit
your insurance information to the SCDMV electronically using the SCALIR system (available at www.sc-alir.com). Commercial carriers and out- of-state agents that do not have access to the SCALIR system can complete the insurance information below and submit to the SCDMV.
Name of Company
NAIC Code |
|
|
Policy Number |
|
Vehicle Coverage Effective |
|
|
To: |
Signature of Authorized Rep. |
|
|
|
|
|
Date Signed |
Telephone |
Vehicle Sold or Traded – If the vehicle on this notice has been sold or traded, you may submit the Notice of Vehicle Sold (SCDMV Form 416), along with this form and mail to the address below or take it into any SCDMV branch office. If you already submitted the Form 416 to the SCDMV to comply with a suspension, you may not submit another one for the same vehicle and suspension. You may submit a Bill of Sale for the vehicle along with this form instead. Form 416 may be accessed on our website at www.scdmvonline.com
Vehicle Repossession (To be completed by the company repossessing the vehicle) – If the vehicle has been repossessed, you may have the company who repossessed the vehicle, provide a letter on company letterhead with the VIN, date of repossession, a phone number and a signature for verification. The company may also fill out an Affidavit for Repossessed Vehicle (SCDMV Form 4034) completed in its entirety and submit along with this form.
Moved Out Of State – If the vehicle no longer resides in South Carolina, you may turn in your SC plates on our website at www.scdmvoline.com or mail them to the address below. If you are trying to clear an FR4 or FR31 suspension, you may submit a copy of your out-of-state registration and this form to the address below and it will be processed in a timely manner. You will receive a letter in the mail from the SCDMV advising if anything else is needed.
Military Service (Military orders or DD-214 must be attached) – If your insurance was cancelled because of military obligations and your vehicle has not been operated upon roads, streets or highways by anyone during the lapse or termination of liability insurance, you must submit a copy of your Military Orders or DD-214 showing the dates of your military service obligations outside the state of South Carolina.
Illness Statement –If your insurance was cancelled because of an illness and your vehicle has not been operated upon roads, streets or highways by anyone during the lapse or termination of liability insurance, you must have your physician complete this section.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Certification of Customer’s Illness |
|
|
|
|
|
|
|
|
|
|
|
|
I certify under penalty of perjury, that the customer listed above was under my care during the dates below. |
|
|
|
|
From: |
To: |
|
|
|
|
|
|
|
|
|
|
Month, Day, and Year |
|
Month, Day, and Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Printed Name |
|
Physician’s Signature |
|
|
Date signed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address, City State, Zip Cpde |
|
|
|
Telephone # |
|
|
Medical ID # |
|
|
|
|
|
|
|
|
|
|
|
SECTION III – CUSTOMER (OWNER) CERTIFICATION |
|
|
|
|
|
|
I certify under penalty of perjury that all the information above is true and correct. |
|
|
|
|
|
|
Customer(Owner) Signature: |
|
|
|
|
|
Date Signed: |
|
|
Documents may be mailed to: SCDMV, Financial Responsibility Office, PO Box 1498, Blythewood, SC 29016-0040
If you checked the military service or illness statement, you cannot wait in a branch office for this to be processed. Please allow 3 to 5 business days for this request to be researched and processed by the FR Compliance Unit. You will be notified by mail advising if anything else is needed.