Our PDF editor can make filling out documents easy. It is quite convenient to enhance the [FORMNAME] document. Check out these actions if you would like do this:
Step 1: Initially, click the orange "Get form now" button.
Step 2: At this point, you're on the file editing page. You can add information, edit existing information, highlight specific words or phrases, place crosses or checks, add images, sign the document, erase needless fields, etc.
These particular segments will constitute the PDF document that you will be completing:
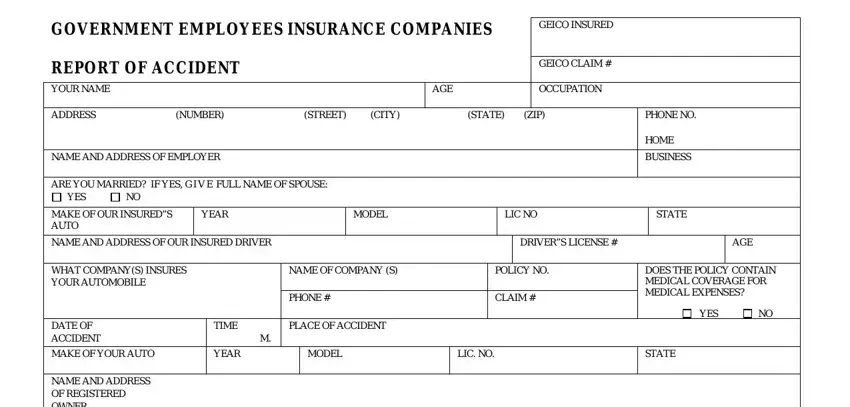
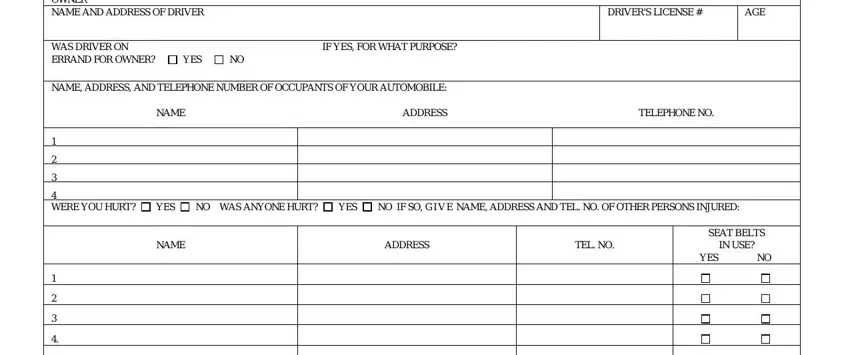
You have to enter the crucial details in the NAME AND ADDRESS OF REGISTERED, DRIVERS LICENSE, AGE, WAS DRIVER ON IF YES FOR WHAT, YES, NAME ADDRESS AND TELEPHONE NUMBER, NAME, ADDRESS, TELEPHONE NO, WERE YOU HURT, YES, NO WAS ANYONE HURT, YES, NO IF SO G I V E NAME ADDRESS AND, and NAME area.
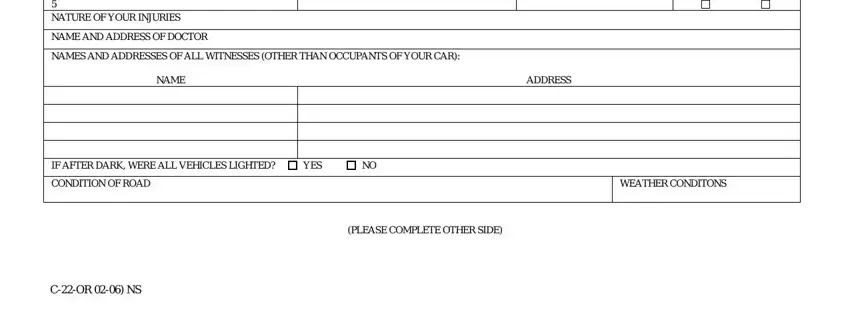
Write the significant details in NATURE OF YOUR INJURIES, NAME AND ADDRESS OF DOCTOR, NAMES AND ADDRESSES OF ALL, NAME, ADDRESS, IF AFTER DARK WERE ALL VEHICLES, YES, CONDITION OF ROAD, WEATHER CONDITONS, PLEASE COMPLETE OTHER SIDE, and COR NS area.
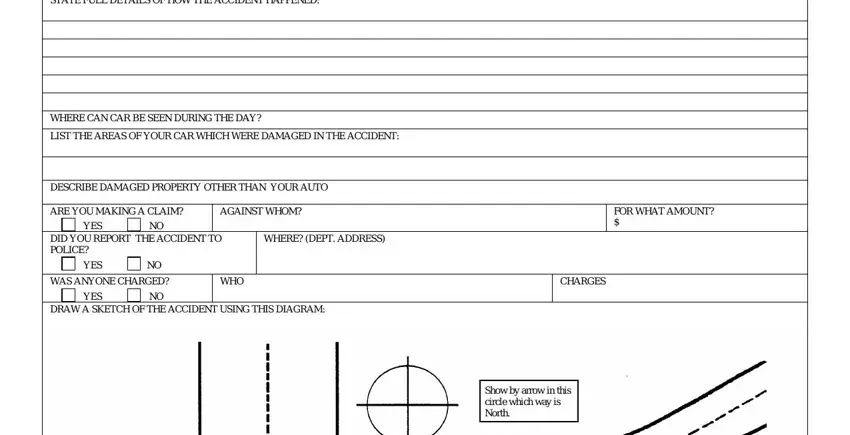
The STATE FULL DETAILS OF HOW THE, WHERE CAN CAR BE SEEN DURING THE, LIST THE AREAS OF YOUR CAR WHICH, DESCRIBE DAMAGED PROPERTY OTHER, ARE YOU MAKING A CLAIM, AGAINST WHOM, YES, DID YOU REPORT THE ACCIDENT TO, WHERE DEPT ADDRESS, YES, WAS ANYONE CHARGED NO, YES, WHO, CHARGES, and DRAW A SKETCH OF THE ACCIDENT field can be used to point out the rights and responsibilities of each party.
Finalize by analyzing the following areas and filling out the pertinent particulars: SIGNATURE, DATE, Any person who knowingly and with, and COR NS.
Step 3: When you click on the Done button, the finalized document is easily exportable to any of your devices. Or alternatively, you will be able to deliver it via mail.
Step 4: Make minimally two or three copies of your form to keep clear of any kind of possible future troubles.
