The idea around our PDF editor was to help it become as easy to use as possible. The general procedure of filling in home health aide time sheets easy should you comply with these steps.
Step 1: The first thing requires you to press the orange "Get Form Now" button.
Step 2: Now you will be on your file edit page. You can include, enhance, highlight, check, cross, insert or remove fields or words.
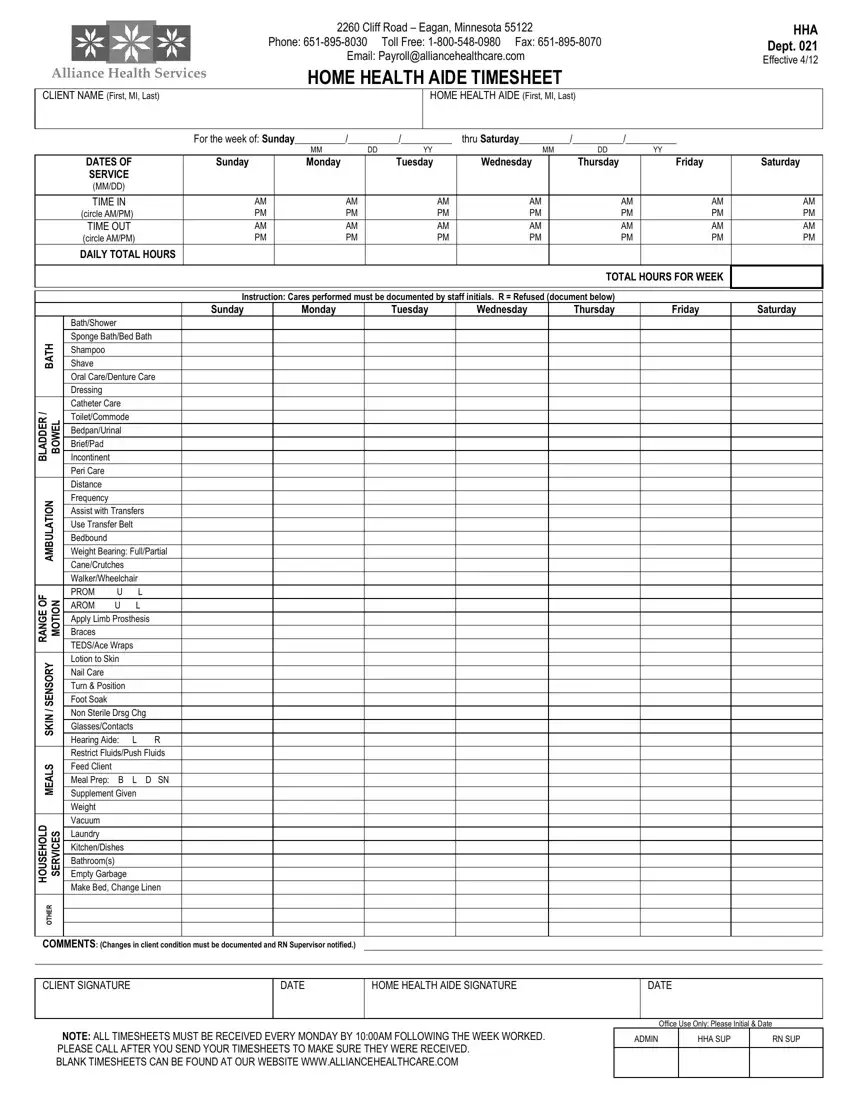
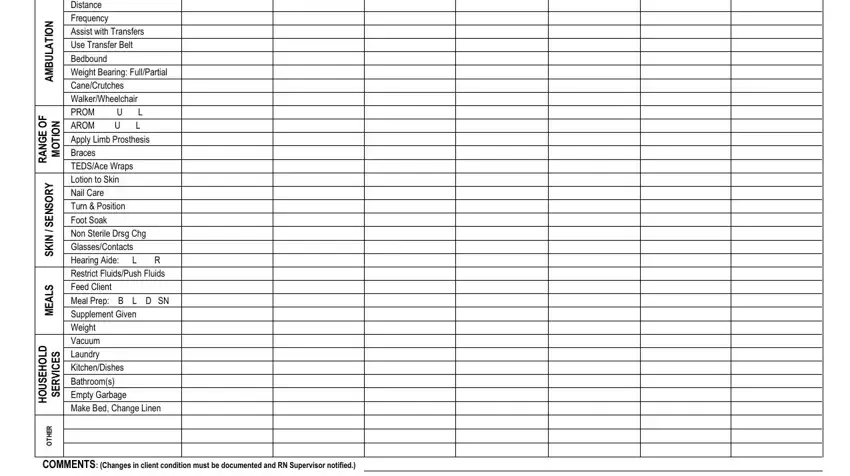
You have to enter the following data to be able to create the template:
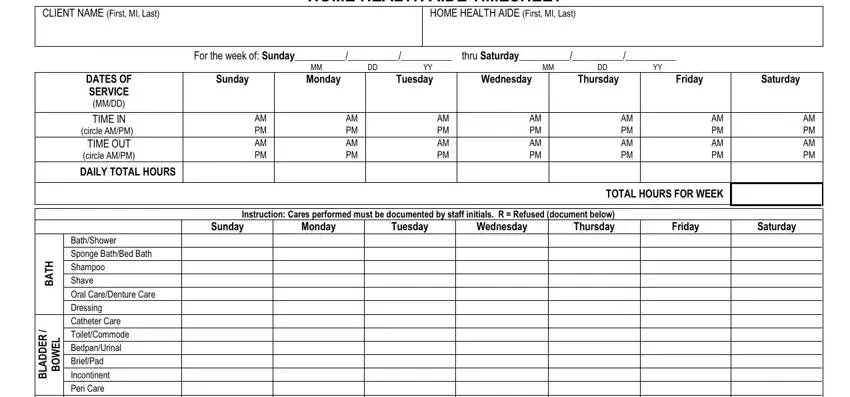
You have to type in the crucial data in the BathShower Sponge BathBed Bath, N O T A L U B M A, F O E G N A R, N O T O M, Lotion to Skin Y R O S N E S, Nail Care Turn Position Foot Soak, N K S, S L A E M, D L O H E S U O H, S E C V R E S, R E H T O, and COMMENTS Changes in client space.
The software will demand you to insert particular fundamental details to automatically complete the part CLIENT SIGNATURE, DATE, HOME HEALTH AIDE SIGNATURE, DATE, NOTE ALL TIMESHEETS MUST BE, BLANK TIMESHEETS CAN BE FOUND AT, Office Use Only Please Initial, ADMIN, HHA SUP, and RN SUP.

Step 3: As soon as you've hit the Done button, your document should be accessible for upload to any kind of gadget or email address you identify.
Step 4: Try to make as many copies of your form as you can to remain away from potential worries.
