This PDF editor makes it easy to prepare documents. You won't have to do much to edit guest away from home application keaystone fill online forms. Basically use these steps.
Step 1: To begin with, pick the orange "Get form now" button.
Step 2: Now you are going to be within the form edit page. It's possible to add, enhance, highlight, check, cross, add or erase fields or text.
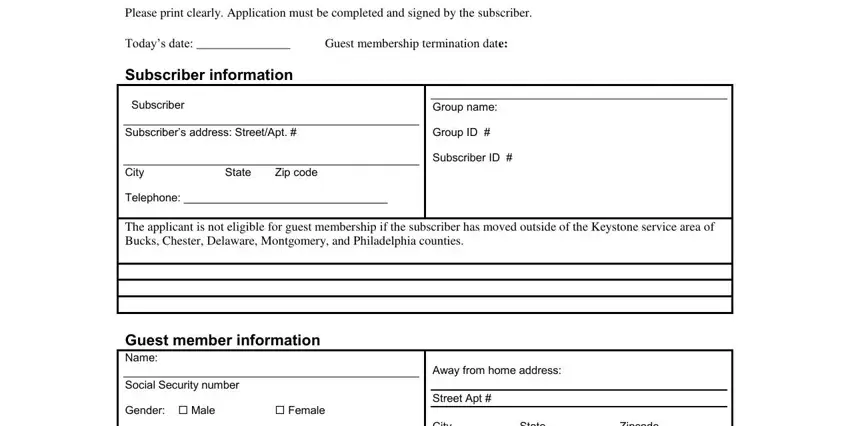
Prepare the memberships PDF and provide the material for each and every area:
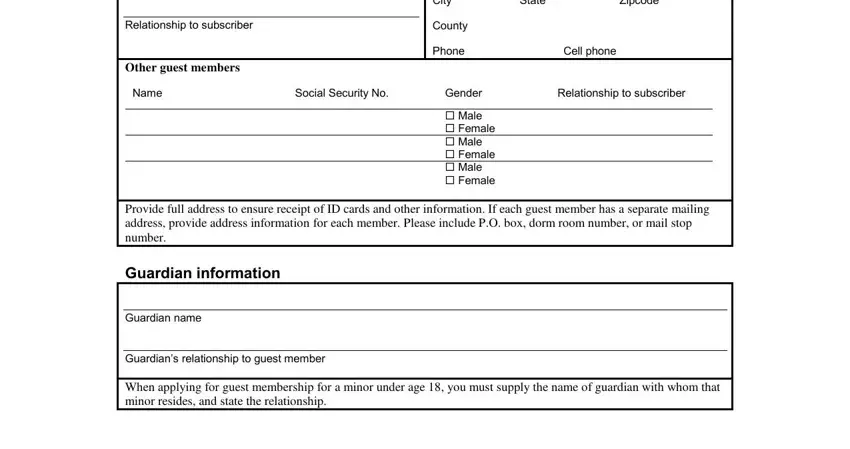
The system will expect you to fill out the City State Zipcode, Relationship to subscriber, County, Other guest members, Phone Cell phone, Name, Social Security No, Gender, Relationship to subscriber, Male Female Male Female Male, Provide full address to ensure, Guardian information, Guardian name, Guardians relationship to guest, and When applying for guest membership box.
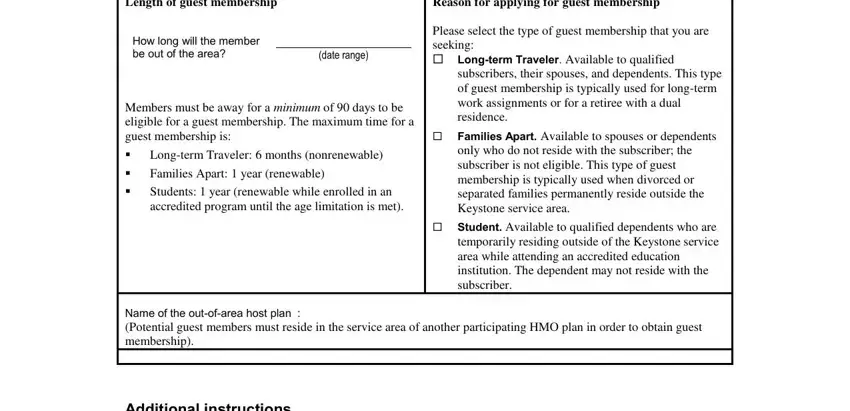
You need to write certain information within the box Guest membership details Length of, How long will the member be out of, date range, Members must be away for a minimum, Longterm Traveler months, Reason for applying for guest, Please select the type of guest, subscribers their spouses and, Families Apart Available to, Student Available to qualified, Name of the outofarea host plan, and Additional instructions.
Be sure to record the rights and responsibilities of the sides in the I hereby certify that all, Subscribers signature, Date, AFHC coordinators use only, Date received, Effective date, and Approved by section.
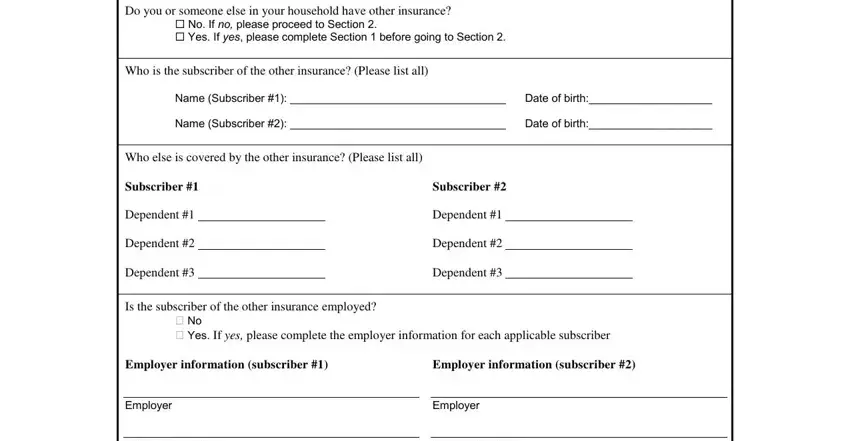
Finish by checking the following sections and filling in the required information: Do you or someone else in your, No If no please proceed to, Who is the subscriber of the other, Name Subscriber Date of birth, Name Subscriber Date of birth, Who else is covered by the other, Subscriber, Dependent, Dependent, Dependent, Subscriber, Dependent, Dependent, Dependent, and Is the subscriber of the other.
Step 3: If you're done, choose the "Done" button to upload the PDF document.
Step 4: In avoiding potential upcoming issues, you need to obtain no less than two or more duplicates of every single file.
