ICE Form I-983 is a document required by U.S. Immigration and Customs Enforcement (ICE) for students on F-1 visas who are applying for or are currently engaged in STEM (Science, Technology, Engineering, and Mathematics) Optional Practical Training (OPT) extensions. This form is filled out collaboratively by the student on an F-1 visa and their employer to outline a detailed training plan that reflects the educational objectives for the student’s development in their field of study.
The purpose of the ICE Form I-983 is to ensure that the STEM OPT extension is educational and directly related to the student’s field of study. It requires detailed information about how the employment will contribute to the student’s professional growth and learning. The U.S. government uses the form to verify that the training provided is legitimate and that it adheres to all the requirements of the STEM OPT program.
Other PDF Forms
Looking for other PDF forms? Check out the selection just below to see what you’ll be able to fill in and edit with our tool. Also, remember that it is easy to upload, fill out, and edit any PDF at FormsPal.
The ICE Form I-983 is comparably lengthy and complicated. That is why you are recommended consulting a specialist prior to completing the document and appending the signatures. Follow the steps below to fill out the form with no mistakes.
The first line is dedicated to your personal information. The applicant has to insert their surname, first name, and middle initial (if there is one), and an email address.
On the second and third lines, you will submit some specific educational data. Input the name of the school, which is recommending the program, its SEVIS school code (including the three-digit suffix), and the name of the school where you have obtained your STEM degree. Then, proceed to provide the designated school’s official name and contact info, your own SEVIS ID number, and the training program requested period (months, dates, years). The authorized dates may not necessarily match actual training dates.
Five statements are presented therein for the trainee to review, acknowledge, and confirm to have understood. An individual should be aware that providing false or misleading information may lead to legal punishment.

If you are ready to establish that the statements above are true and correct, append your signature (in ink only), provide your name in print, and date the paper.
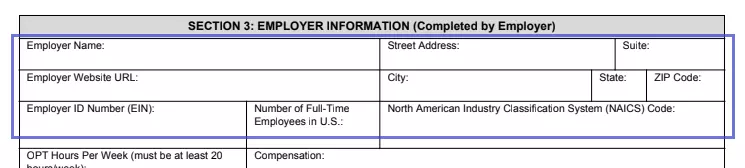
The third section is filled out by the employer. Initially, enter your company name, street address, suite, city, state, zip code, and website URL (if available). Provide your EIN, the number of full-time staff members in the US, and the NAICS code.

Hereunder is the info concerning your student-employer agreement. Indicate the number of hours per week you are hiring the student for (at least 20) and the start date of employment.
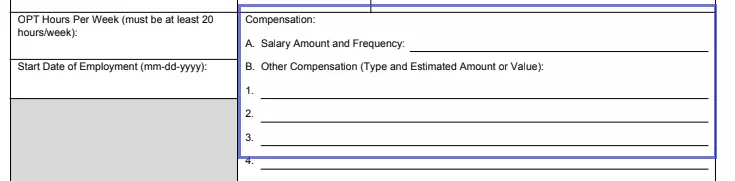
The compensation conditions are provided as well. Insert the amount of salary (or stipend) you will pay the trainee and the frequency of these payments. Keep in mind that the terms and conditions of the program opportunity have to commensurate with those applicable to other US workers.

In this section, the employer official with signatory authority appends the signature, stating that they have reviewed the four statements therein and confirm them to be true and correct.

Pay special attention to the fact that the DHS may conduct a visit to your institution to ensure that the STEM OPT training program requirements are being met.
The training plan is completed by both the student and the employer.

The first two lines have to be filled out with both parties’ names.

After that, proceed to indicate more info about the employer site. The site name may be the same as provided in Section 3, or, if the employer is a large company with several branches, be different. The address where the applicant is supposed to do their training course is inserted thereafter. An official who will be responsible for monitoring the student’s performance is about to be named then, along with their email, title, and phone number are also entered.
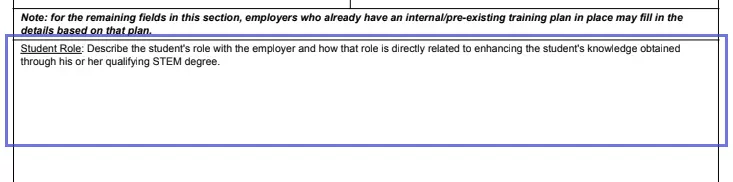
Taking the STEM degree, you possess into account. The employer must describe what tasks and assignments you will carry out during the STEM OPT.

Each student enters the program to eventually reach specific goals and objectives. The employer should describe what skills, knowledge, and techniques the student will learn to apply and how much time it will take.

The trainee’s work will obviously be supervised. Describe the methods the employer intends to use to monitor the student’s performance herein.

Explain how the employer measures and evaluates the work you are doing as an F-1 student.

If there are any additional remarks to mention, indicate them in a special box.

As well as the other parties of the agreement, the official representative of the company, which is hiring an F-1 student to complete a STEM OPT, has to look through the statements they are about to confirm and sign and date the document.
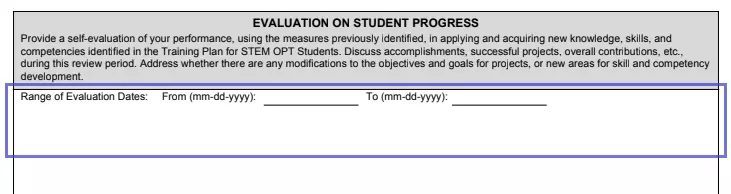
Each STEM OPT participant has to evaluate themselves annually, using the measures described in the previous section. You are supposed to discuss the accomplishments, successful projects, and overall contribution to the company with the other employee liable for controlling your work. Complete the box with the information about the results you have achieved. Your mentor will check this data and append their signature to affirm that they agree with the evaluation.
The trainee must complete the final evaluation after the training has been finished. In this box, you will describe all knowledge, practical skills, competencies, and any other important accomplishments you had during the review period. Likewise, the annual evaluation, the final one, has to be checked and affirmed by your supervisor. Both of you must print your names, date the form, and append your signatures in ink to establish that the training course has been completed satisfactorily.