
It's super easy to fill in the illinois form 45. Our PDF editor was built to be easy-to-use and let you prepare any document easily. These are the actions to go through:
Step 1: Hit the button "Get form here" to get into it.
Step 2: As you access our illinois form 45 editing page, you will find all of the actions it is possible to take with regards to your file within the upper menu.
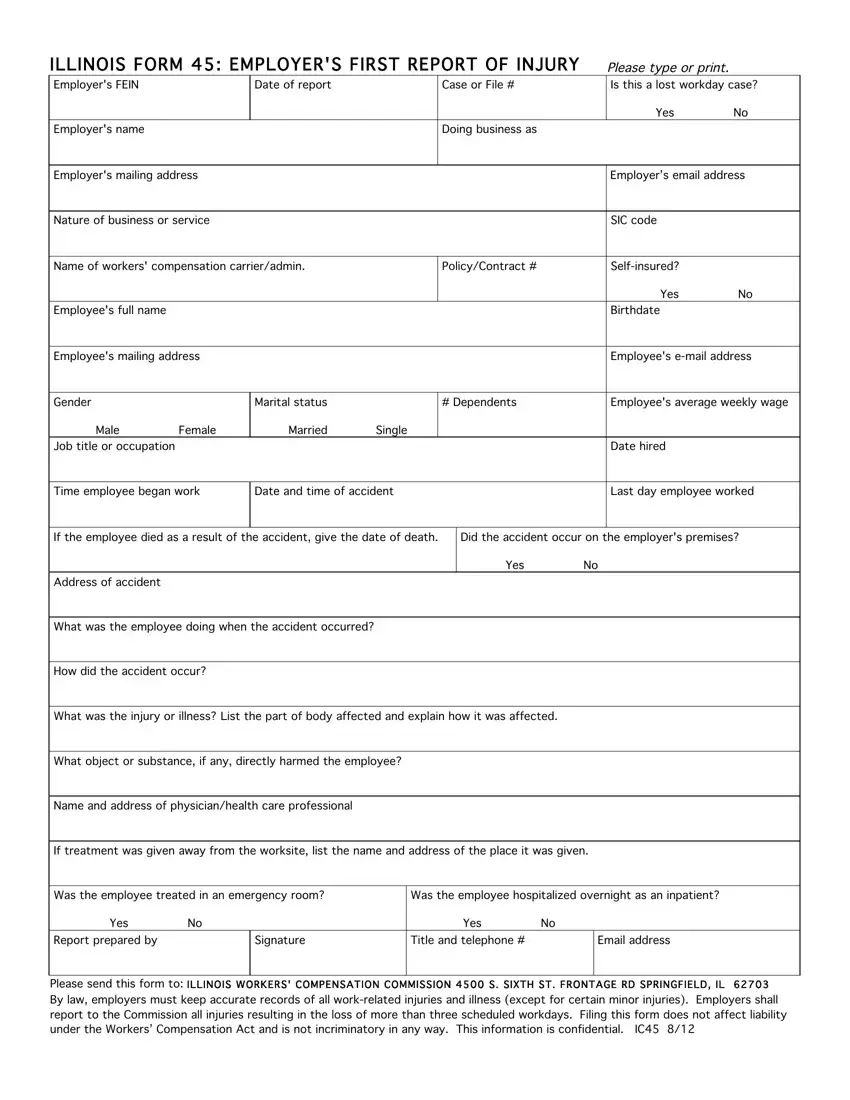
Make sure you provide the following details to prepare the illinois form 45 PDF:
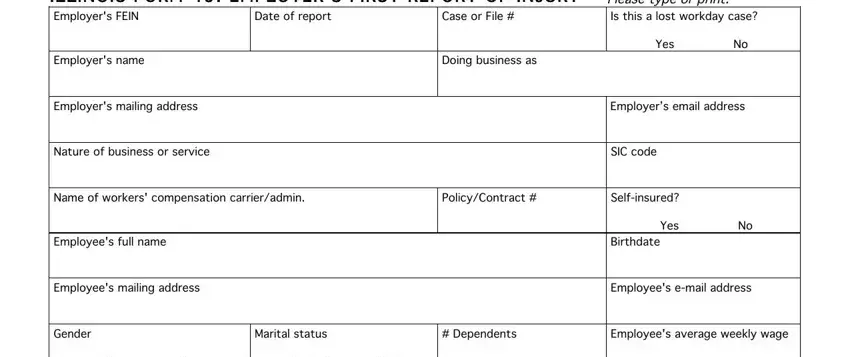
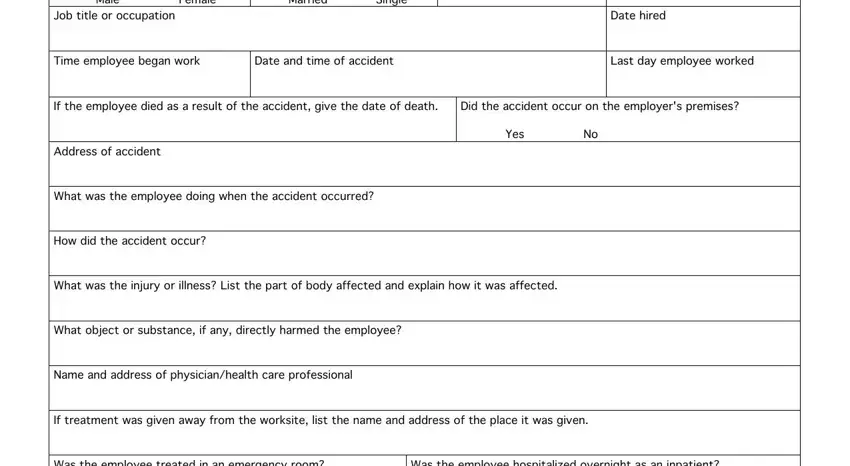
Complete the Male Female Job title or occupation, Married Single, Date hired, Time employee began work, Date and time of accident, Last day employee worked, If the employee died as a result, Did the accident occur on the, Yes No, Address of accident, What was the employee doing when, How did the accident occur, What was the injury or illness, What object or substance if any, and Name and address of section using the particulars requested by the program.
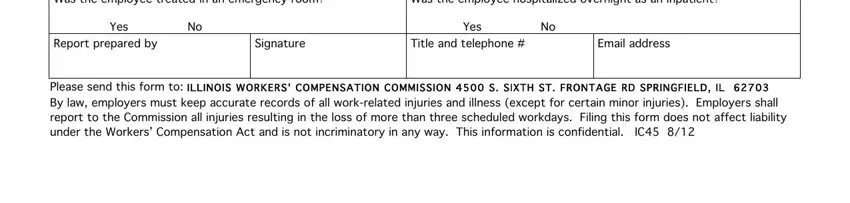
Note the vital information in Was the employee treated in an, Was the employee hospitalized, Yes No Report prepared by, Signature, Yes No Title and telephone, Email address, and Please send this form to ILLINOIS segment.
Step 3: Press "Done". It's now possible to upload your PDF file.
Step 4: Generate a copy of each separate file. It will save you some time and make it easier to stay away from misunderstandings as time goes on. By the way, your information won't be used or analyzed by us.
