The PDF editor was created with the aim of allowing it to be as effortless and intuitive as possible. All of these actions will make creating the illinois school sports physical form easy and quick.
Step 1: The following webpage has an orange button that says "Get Form Now". Merely click it.
Step 2: The form editing page is now open. You can include text or enhance current data.
Complete the illinois school sports physical form PDF and enter the content for every area:
Write down the requested details in chest, during, exercise exercise, ECG, EKG, echo, cardiogram expected, during, exercise friends, during, exercise Yes, implanted, defibrillator seizures, or, near, drowning joints, Yes, or, legs, after, being, hit, or, falling hit, or, falling lose, weight cancer, and doctor box.
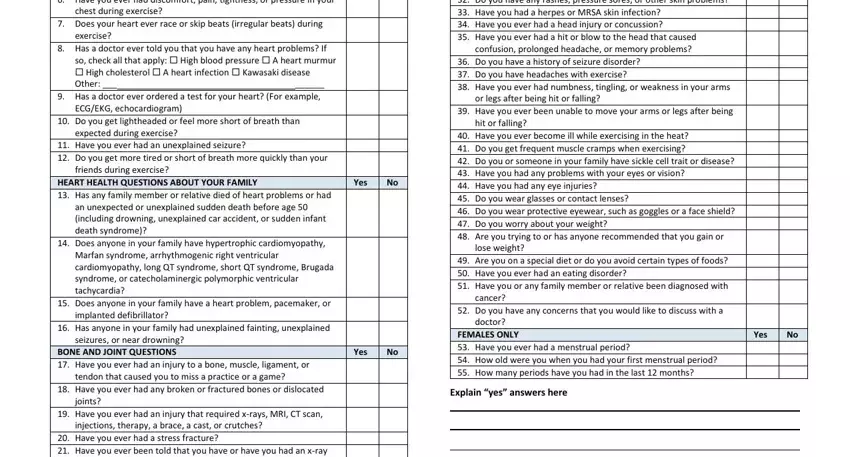
The program will require you to insert some necessary info to instantly fill in the part red, disease, Signature, of, parent, guardian Date, and Explain, cid, cide, sci, dans, we, cid, she, cide

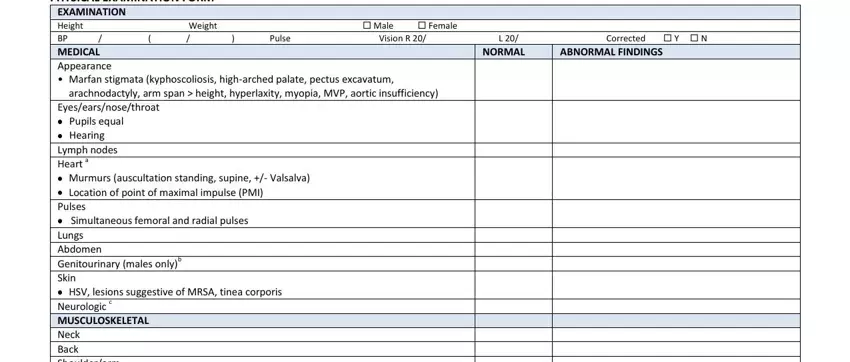
You will need to identify the rights and responsibilities of every party in part PHYSICAL, EXAMINATION, FORM ABNORMAL, FINDINGS and NORMAL.
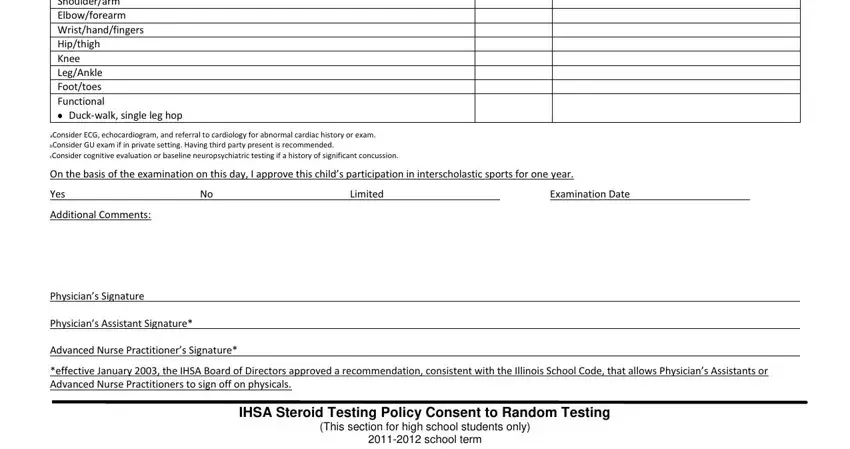
Fill in the file by reviewing these areas: Yes, Limited, Examination, Date and school, term
Step 3: Press the "Done" button. Now, you may transfer the PDF file - upload it to your device or send it by means of email.
Step 4: It's possible to make duplicates of the file toremain away from any upcoming problems. You need not worry, we cannot distribute or check your information.
