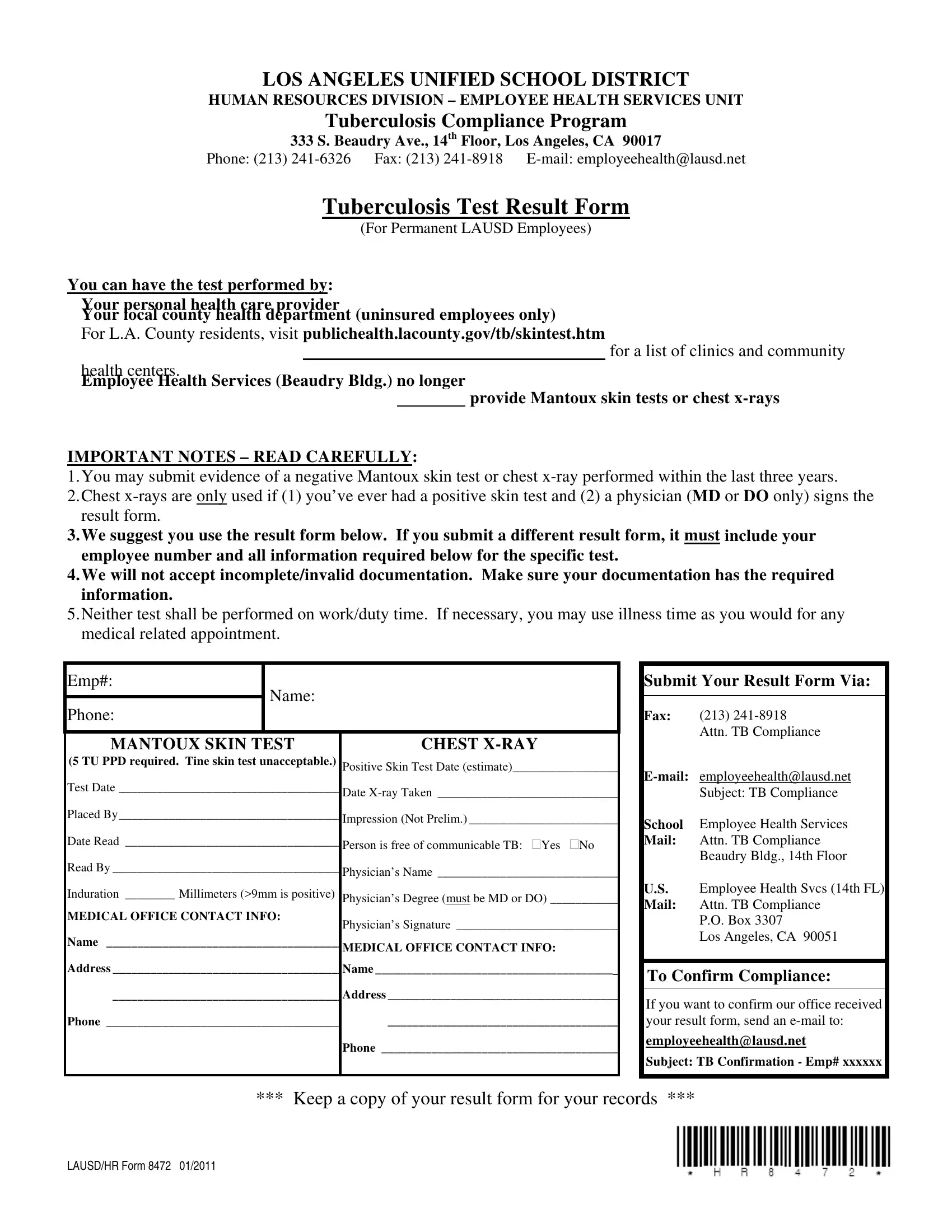
In an effort to ensure the health and safety of its educational environment, the Los Angeles Unified School District (LAUSD) mandates that all permanent employees comply with its Tuberculosis (TB) Compliance Program, facilitated by the Human Resources Division's Employee Health Services Unit. Located at 333 S. Beaudry Ave., 14th Floor, Los Angeles, CA 90017, the unit oversees the TB Test Result Form, also known as the LAUSD HR Form 8472, a critical document that consolidates TB testing results. Employees have the flexibility to undergo TB testing either through their personal healthcare providers, at local county health departments (specifically for uninsured employees), or via other prescribed channels, albeit Employee Health Services no longer offers Mantoux skin tests or chest x-rays. The form meticulously outlines the prerequisites for test documentation, including a negative Mantoux skin test or chest x-ray result within the last three years, with specific instructions for cases of previously positive skin tests. The form emphasizes the necessity of submitting complete and valid documentation, bearing the employee’s number and precise test result information, to avoid rejection. Additionally, it underlines that neither the Mantoux skin test nor chest x-ray should be performed during work or duty hours, allowing the usage of illness time for such medical appointments if needed. Instructions for submitting the form, along with contact information for confirmation of receipt, are clearly provided to aid in compliance. This measure underscores LAUSD's commitment to maintaining a TB-free environment for its staff and students.
| Question | Answer |
|---|---|
| Form Name | Lausd Hr Form 8472 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | lausd tb risk assessment form, lausd tb compliance, E-mail, employeehealthlausd |